| disease | Noise-induced Deafness |
| alias | Chronic Vocal Injury |
Noise-induced deafness is a slow, progressive sensorineural hearing loss caused by prolonged exposure to noise stimulation.
bubble_chart Etiology
When the noise exceeds an intensity of 85–90 dB, it causes damage to the cochlea. The extent of the damage is related to the following factors:
1. Noise intensity: The incidence of noise-induced deafness increases with the rise in noise intensity.
2. Noise spectrum characteristics: Under the same intensity conditions, high-frequency noise causes more severe hearing damage than low-frequency noise; narrow-band noise or pure tones inflict greater hearing damage than wide-band noise.
3. Noise type: Impulse noise is more harmful than steady-state noise.
4. Exposure duration and mode: Continuous exposure causes more injury than intermittent exposure; the longer the exposure to noise, the more severe the hearing injury; the closer the proximity to the noise source, the more susceptible the hearing is to damage.
5. Individual susceptibility: Older individuals, those with weaker constitutions, or those who have previously suffered from sensorineural deafness are more vulnerable to noise injury. However, opinions differ regarding the impact on those with middle ear diseases—some suggest that perforated eardrums or interrupted ossicular chains may result in relatively milder noise-induced damage.
bubble_chart Pathological Changes
Due to the long-term effects of noise stimulation, the hair cells in the inner ear are damaged, and the spiral organ and spiral ganglion undergo degenerative changes. The most pronounced lesions occur at the terminal segment of the basal turn of the cochlea and the beginning of the second turn, which corresponds to the area receiving 4000Hz sound stimulation. This region is particularly susceptible to noise injury, possibly because it is close to the tympanic cavity and located in an area with relatively poor blood circulation between the two windows. Another theory suggests that this is the point where low-frequency and high-frequency sound waves meet, creating increased tension due to their opposing directions, which can easily lead to local tissue deformation. Additionally, some believe this is related to the resonance physiology of the external auditory canal, as the resonant frequency of the external auditory canal is around 3000–4000Hz, thereby amplifying the harm of noise at this frequency to the inner ear. Animal experiments with noise stimulation have shown that inner ear damage primarily affects the cochlear duct and saccule, while the utricle is less affected, and the semicircular canals remain unharmed.
bubble_chart Clinical Manifestations1. Progressive hearing loss
When initially exposed to noise, hearing becomes slightly dull. If the noise is removed, hearing recovers within minutes. This phenomenon is called auditory adaptation. Under prolonged and intense noise exposure, hearing becomes significantly dull, taking several hours to recover, which is then termed auditory fatigue. Further noise exposure can lead to hearing injury, which is difficult to recover from spontaneously. Early stages show hearing impairment at 4000Hz. The audiogram exhibits a V-shaped dip, which gradually deepens over time, affecting 2000Hz and 8000Hz as well, eventually leading to a descending slope in hearing (Figure 1). Typically, the curves are symmetrical in both ears; asymmetry often indicates additional ear conditions or specific individual circumstances.
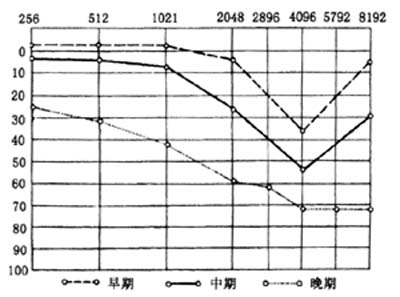
Figure 1: Air conduction audiogram of noise-induced deafness
2. Tinnitus
May appear before deafness or develop simultaneously, characterized by high-pitched sounds, often disturbing day and night.
3. Systemic reactions
May include headache, dizziness, insomnia, fatigue, memory decline, slow response, depression, palpitations, elevated blood pressure, nausea, loss of appetite, and indigestion.
bubble_chart Treatment Measures
In the early stages, if hearing loss is only at 4000Hz, resting for several days or weeks and using vitamins and vasodilators may help restore hearing. However, if the condition has persisted for a long time, leading to degeneration of the spiral organ and spiral ganglion cells, treatment is unlikely to be effective. In such cases, hearing aids can be used to assist with daily life.
1. Controlling the Noise SourceThis is the most proactive and fundamental approach. When constructing factory buildings and installing machinery, various soundproofing, vibration-damping, and sound-absorbing measures should be adopted. For example, noisy workshops should be separated from other factory buildings, with trees planted in between; the walls and smallpox panels of the workshop should be equipped with sound-absorbing materials; machines should be installed with appropriate spacing; appropriate filling materials should be used between machines and foundations, as well as between metal surfaces; pipeline noise can be mitigated by wrapping methods, and airflow noise can be reduced with mufflers or by enlarging exhaust ports, thereby reducing noise to within the national protective standards (85–90 dB).
2. Reducing Exposure Time
Taking breaks in soundproof rooms or reducing daily or weekly exposure to noise can also lower the incidence of hearing damage. Job rotation based on actual conditions can further reduce hearing impairment.
3. Ear Protection
Use protective equipment such as earplugs, earmuffs, or soundproof helmets. Generally, simple earplugs should be worn when working long-term in an 80 dB noise environment; for noise levels above 90 dB, protective gear is mandatory. A simple method involves tightly plugging the ear canal with cotton coated in Vaseline, which can provide up to 30 dB of sound insulation.
4. Health Monitoring
Hearing should be checked before employment. Individuals with sensorineural deafness or noise sensitivity should avoid working in high-noise environments. Regular hearing tests should be conducted for those exposed to noise to detect early hearing injuries promptly and provide appropriate treatment.
5. Seeking Early Treatment


