| disease | Paronychia |
The proximal part of the nail (nail root) is closely connected to the skin, which extends distally along both sides of the nail, forming the nail groove. Paronychia is an infection of the nail groove or its surrounding tissues. It is often caused by minor punctures, contusions, hangnails, or cutting the nails too deeply, with Staphylococcus aureus being the most common pathogen.
bubble_chart Clinical Manifestations
Initially, the subcutaneous tissue on one side of the nail becomes red, swollen, and painful. Some cases may resolve spontaneously, while others rapidly progress to suppuration. The pus spreads from one side of the nail groove to the subcutaneous tissue at the nail root and the opposite nail groove, forming a semi-circular abscess. Paronychia usually presents no systemic symptoms. If not incised and drained, the abscess may extend beneath the nail, becoming a subungual abscess (Figure 1), where yellowish-white pus can be seen separating the nail from the nail bed. Subungual abscesses can also result from direct puncture wounds to the nail or infection of traumatic hematomas beneath the nail. If inadequately treated, it may develop into chronic paronychia or chronic osteomyelitis of the phalanx. In chronic paronychia, a small sinus opening appears beside the nail groove, with granulation tissue protruding outward. Chronic paronychia may sometimes be complicated by fungal infection.
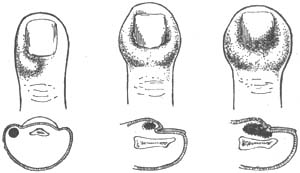
Figure 1 Subungual abscess
1. The proximal side of one or both nail grooves of the finger or toe becomes red, swollen, and painful, followed by the appearance of pus points. After pus discharge, granulation tissue can be seen.
2. When the infection spreads to the nail bed, local pus accumulation can cause the entire fingernail or toenail to lift and fall off.bubble_chart Treatment Measures
In the early stages, warm compresses, physical therapy, topical application of ichthammol ointment or Sanhuang Powder, and the use of sulfonamides or antibiotics can be applied.
If pus has already formed, a longitudinal incision can be made at the nail groove for drainage. When the infection has spread to the subcutaneous area around the base of the nail, longitudinal incisions can be made on both sides of the nail groove, the nail root flap can be lifted, the nail root can be excised, and a small piece of Vaseline gauze or latex sheet can be placed for drainage. If pus has accumulated under the nail bed, the nail should be removed, or the portion of the nail covering the abscess should be trimmed. During nail removal, care should be taken to avoid injury to the nail bed to prevent deformity of the newly grown nail in the future.
Cutting nails should not be too short. If there is a small wound on the finger, apply iodine tincture and wrap it with sterile gauze to prevent infection.



