| disease | Flat Feet |
Flatfoot is a deformity characterized by a lowered or absent longitudinal arch of the foot. Flatfoot caused by ligament laxity is common in adolescents and has a genetic predisposition.
bubble_chart Pathogenesis
The cause of the disease remains unclear, but epidemiological studies have found a clear genetic predisposition. Pathological observations reveal no developmental deformities in the tarsal bones, but the ligaments of the joint capsules connecting the talocalcaneal, talonavicular, and naviculocuneiform joints are looser than normal. This causes the calcaneus to internally rotate beneath the talus during weight-bearing, with its anterior end shifting dorsally and laterally, while the talus shifts toward the metatarsal and medial side. As a result, the already lax calcaneonavicular metatarsal ligament becomes even more relaxed, failing to support the talar head and leading to a lowered longitudinal arch of the foot. The loosening of the calcaneotalar ligament further exacerbates calcaneal valgus, worsening the collapse of the longitudinal arch.
bubble_chart Clinical Manifestations
Young children are often asymptomatic. It is usually only when abnormal wear on the soles of their shoes is noticed that parents become aware of the issue. In children with obesity and adolescent patients, prolonged standing may lead to plantar pain and discomfort in the lower legs. Typically, the foot arch is present when not bearing weight, but weight-bearing examination reveals a lowered or absent longitudinal arch. Clinically, it can be divided into three types, all of which require observation of changes in the longitudinal arch under weight-bearing conditions: - Mild: The longitudinal arch is lowered. - Moderate: The longitudinal arch disappears. - Severe: The longitudinal arch disappears, accompanied by a convex medial edge of the foot and displacement of the talus toward the metatarsal side, i.e., anterior and inferior to the medial malleolus. Patients may sometimes exhibit Achilles tendon shortening and hindfoot valgus.
X-ray examination should be performed under weight-bearing conditions, with anteroposterior and lateral views of the foot. The primary focus is on measuring changes in the arch angle on the lateral view: 1. Draw a straight line along the central axis of the talus, navicular, first cuneiform, and metatarsal bones. Then, draw another line from the center of the navicular bone parallel to its anterior and posterior articular surfaces, intersecting the first line. Normally, these two lines form a right angle (Figure 29). If pathology or ligament laxity occurs at the talonavicular joint, the central axes of the navicular, first cuneiform, and metatarsal bones will not align with the talar axis, forming an angle on the metatarsal side. The talar axis will pass through the lateral fourth of the navicular bone (Figure 29B). If ligament laxity occurs at the naviculocuneiform joint, the talar axis will lie on the metatarsal side of the first cuneiform, intersecting the perpendicular line from the navicular center at a right angle (Figure 29C). If the line through the navicular center extends anteriorly and posteriorly, lying on the metatarsal side of both the talus and first metatarsal, it indicates ligament laxity at both the talonavicular and naviculocuneiform joints (Figure 29A). 2. **Talar plantarflexion angle**: Draw a horizontal line along the metatarsal side and intersect it with the talar axis. The normal value is 26.5° ± 3.5°. An increased angle indicates talar plantarflexion deformity. 3. **Talonavicular dorsoplantar angle**: On a weight-bearing anteroposterior view, draw a line parallel to the distal articular surface of the navicular bone and another line along the talar axis. The medial angle formed by these lines is the talonavicular dorsoplantar angle. The normal range is 60°–80°. An angle >60° indicates talar displacement.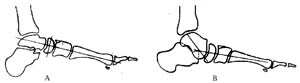
**Figure 29** Weight-bearing lateral foot radiograph measuring the talus-metatarsal angle.
bubble_chart Treatment Measures
Individuals with mild or moderate asymptomatic flat feet do not require treatment. In the past, walking barefoot on sandy beaches or grassy fields was encouraged to train the muscles of the lower legs and feet, enhance the stability of the tarsal joints, and elevate the longitudinal arch. Various orthopedic shoes were also recommended in hopes of correcting flat feet. However, practice has shown that these measures do not have a corrective effect on flat feet; they can only alleviate local discomfort and pain. Therefore, for symptomatic moderate to severe flat feet in children under 10 years old, passive or active stretching of the triceps surae can be employed to relieve discomfort in the lower legs and feet caused by muscle spasms. Wearing Thomas orthopedic shoes with a 0.3–0.6 cm thickened medial heel or adding a 0.5–0.75 cm longitudinal arch support inside the shoe can reduce or eliminate pain and discomfort, though these measures do not correct the deformity.
If non-surgical treatments fail to relieve pain and the condition affects weight-bearing, walking, or wearing shoes in moderate to severe flat feet patients over 10 years old, surgical intervention is indicated. Surgical methods include soft tissue procedures such as tendon transfers and ligament tightening, as well as bony procedures such as tarsal joint fusion, triple arthrodesis, and tarsal osteotomy. However, isolated soft tissue procedures or single tarsal joint fusions have been abandoned due to poor outcomes. Currently, a combination of soft tissue and bony procedures is preferred, significantly improving efficacy.

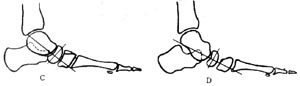
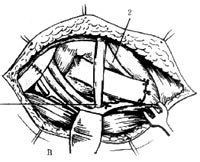
**Figure 30** Formation of the joint capsule and ligament-bone flap on the medial side of the talus, navicular, and cuneiform bones.
1. Tibialis posterior tendon 2. Calcaneonavicular and metatarsal ligament 3. Tibialis anterior tendon
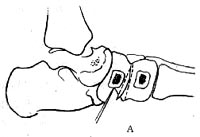
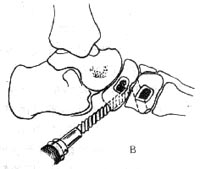
**Figure 31** A. Excision of the naviculocuneiform joint cartilage B. Drilling holes on the plantar side of the navicular and cuneiform bones
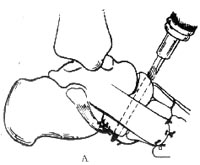
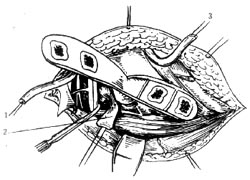
**Figure 32** A. After suturing the joint capsule and ligament-bone flap, drilling from the dorsal navicular to the plantar side B. Fixation of the tibialis anterior and posterior tendons through the navicular bone tunnel 1. Tibialis anterior and posterior tendons 2. Tibialis anterior tendon sheath
Lax talocalcaneal joint flatfoot often presents with obvious calcaneal valgus deformity. In immature patients, the Grice extra-articular subtalar arthrodesis can correct the flatfoot without affecting longitudinal foot growth. This procedure involves exposing the sinus tarsi through an oblique incision anterior to the lateral malleolus, removing cortical bone from the sinus tarsi, packing it with autogenous cancellous bone strips, and fixing with a screw. Postoperative gypsum external fixation is maintained until bone graft healing occurs. For older children or adolescents, triple arthrodesis is also a recommended method.
Flat feet can be divided into two main categories: primary and secondary. When diagnosing primary flat feet caused by ligament laxity, a thorough differential diagnosis should be performed to exclude flat feet resulting from accessory navicular bone deformity, first metatarsal shortening, or congenital clubfoot post-surgical complications. Additionally, neuromuscular conditions such as paralytic flat feet caused by poliomyelitis or spastic flat feet due to cerebral palsy must be ruled out. A correct diagnosis can usually be made based on the age of onset, detailed medical history, physical examination, and X-ray findings.


