| disease | Wear and Tear |
| alias | Abrasion |
The chronic wear of hard dental tissues caused solely by mechanical friction is called attrition. Uniform and appropriate attrition is of significant importance to the health of periodontal tissues. For example, the wear of cusps reduces lateral pressure during mastication, allowing the morphology of the cusps to adapt to the function of the periodontal tissues. Additionally, the wear of the tooth crown can reduce the length of the clinical crown, maintaining a harmonious balance between crown and root length, thereby preventing excessive burden on the periodontal tissues due to leverage effects.
bubble_chart Etiology
Wear can occur during normal chewing, and this physiological wear is called masticatory wear. Other types of tooth wear not caused by normal chewing processes are pathological phenomena, collectively referred to as non-masticatory wear.
bubble_chart Pathological Changes
A dead tract or transparent layer forms in the exposed dentin area; reparative dentin develops in the pulp cavity corresponding to the exposed dentin; and the pulp undergoes dystrophic changes. The amount of reparative dentin formed depends on the area of exposed dentin, the duration of exposure, and the pulp's response. As reparative dentin forms, the volume of the pulp cavity may gradually decrease.
bubble_chart Clinical Manifestations
1. Attrition Wear Also known as attrition, it generally occurs on the occlusal surface (Figure 1) or incisal edge, but can also occur on other tooth surfaces in cases of malaligned dentition. Since deciduous teeth remain in the mouth for a shorter time than permanent teeth, their degree of attrition wear is less pronounced than that of permanent teeth. Several years to decades after the eruption of permanent teeth, noticeable attrition wear appears on the occlusal surfaces of posterior teeth and the incisal edges of anterior teeth. Initially, small smooth facets appear on the cusps or ridges of the teeth, and the incisal edges become slightly flattened. With age, attrition wear becomes more pronounced, tooth height decreases, occlusal slopes flatten, and the mesiodistal diameter of the teeth diminishes. In certain areas of the teeth, the enamel may be completely worn down, exposing the dentin and forming sharp edges. During mastication, slight mobility of each tooth causes adjacent teeth to rub against each other at their contact points, leading to wear that transforms point contacts into surface contacts. This can easily result in food impaction, interproximal caries, and periodontal disease.
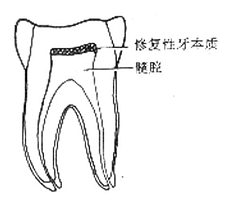
Figure 1 Occlusal Wear
The degree of wear depends on tooth hardness, food hardness, chewing habits, and masticatory muscle tension. The extent of wear is directly proportional to the patient's age, food abrasiveness, and chewing force, and inversely proportional to tooth hardness.
2. Non-Attrition Wear This refers to the pathological loss of tooth hard tissue caused by abnormal mechanical friction. Bad habits and certain occupations are common causes of such wear. Examples include women using their teeth to open hairpins, or carpenters, shoemakers, and tailors frequently holding nails, needles, or threads with their teeth. Bruxism can also lead to severe wear.
1. Medical History: Pay attention to any systemic diseases, such as gastrointestinal dysfunction, neurasthenia, xerostomia; and habits like chewing hard foods or poor oral habits, such as unilateral chewing.
2. Clinical Manifestations: Partial enamel wear exposes light yellow dentin, which may lead to tooth sensitivity. Complete enamel wear can result in pulp diseases or pulp cavity occlusion. Uneven wear may cause occlusal trauma, food impaction, and damage to periodontal tissues and mucous membrane. Severe wear of all teeth may also lead to temporomandibular joint disorders.
3. Auxiliary Examination: Dental X-rays can be taken to assess the relationship of the pulp cavity.
bubble_chart Treatment Measures
1. Physiological wear requires no treatment if asymptomatic.
2. Remove and correct the causes of pathological wear.
3. Desensitization treatment should be performed for dentin hypersensitivity.
4. For uneven wear, appropriate occlusal adjustment is needed to grind down sharp cusps and edges.
5. For pulp and periapical diseases, follow standard procedures for pulp and periapical treatment.

6. For food impaction, restore normal contact relationships and reconstruct occlusal spillways. In cases of severe wear with temporomandibular joint syndrome, overlay dentures should be used to restore vertical occlusal dimension.
Wear can also cause various complications or become a pathogenic factor.
1. Dentin hypersensitivity This symptom of soreness may gradually lessen and disappear over several months; sometimes, it can persist for a longer time without improvement. The degree of sensitivity often varies from person to person. Generally speaking, the faster the wear process and the larger the exposed area, the more pronounced the soreness.
2. Food impaction When chewing food, the occlusal surface morphology established by marginal ridges and developmental grooves usually helps divert food away from interdental spaces. After tooth wear, flat surfaces replace normal convexities, increasing the tendency of cusps to wedge food into opposing interdental spaces. Shortened tooth crowns due to wear and proximal surface wear can also lead to food impaction, promoting periodontal disease and proximal caries.
3. Pulp and periapical lesions These are caused by excessive wear exposing the pulp cavity.
4. Temporomandibular joint disorder syndrome Severe occlusal wear can lead to reduced vertical dimension of occlusion, resulting in temporomandibular joint damage.
5. Traumatic occlusion Uneven wear can leave steep cusps, leading to traumatic occlusion.
6. Traumatic ulcer Overly sharp cusps and edges left by uneven wear can irritate the buccal or lingual mucosa, causing local ulcers.


