| disease | Duplication of Kidney and Ureter |
Duplication of the kidney and ureter is a common congenital malformation of the urinary system. This anomaly can be unilateral or bilateral, with unilateral cases being more frequent than bilateral ones. The right side is affected four times more often than the left, and it is more common in females than in males. Reported incidence rates vary. Campbell's autopsy study of 51,880 cases identified 342 instances of ureteral duplication, a ratio of 1:160. In contrast, Nordmark found 138 cases among 4,774 radiographic examinations, a ratio of 1:35. Thompson and Amar reported that 6% of patients undergoing urography for urinary tract issues exhibited ureteral duplication. Swenson and Ratner detected 62 cases in 4,000 pediatric urograms, a ratio of 1:64. Overall, these statistics indicate that duplication of the kidney and ureter is far from a rare congenital anomaly. Additional data suggest that in females, the incidence of complete and incomplete ureteral duplication is roughly equal, whereas in males, incomplete duplication predominates.
bubble_chart Pathogen
On the sixth day of the human embryo's day and night cycle, a small blind tube called the ureteric bud protrudes dorsally from the end of the mesonephric duct (Wolffian duct) where it enters the cloaca. The ureteric bud grows rapidly, with its tip enveloped by primitive nephrogenic tissue, resembling a broad bean. The ureteric bud develops into the renal pelvis, which branches to form the renal calyces, further branching into minor calyces and collecting ducts. If branching occurs prematurely, it results in duplicated ureteral anomalies. The level and extent of branching determine whether the anomaly is complete or incomplete, double or multiple. Duplicated ureters are often accompanied by duplicated kidneys. Most duplicated kidneys are fused into a single mass with a common membrane and a shallow groove on the surface, but the renal pelvises, ureters, and blood vessels remain separate. Complete separation of duplicated kidneys is very rare.
bubble_chart Pathological ChangesThe duplicated kidney is usually fused into a single mass, larger than a normal kidney. The two kidneys are often arranged vertically, rarely side by side or front-to-back, and seldom completely separated. In the vertical arrangement, the upper kidney is usually smaller with only one calyx, while the lower kidney is larger, often possessing two calyces. If the connected ureter is a complete-type duplex ureter, the ureter linked to the lower kidney typically enters the bladder at the normal ureteral orifice position. In contrast, the ureter connected to the upper kidney enters the bladder below the normal ureteral orifice position, within the trigone of the bladder. In males, it may open into the posterior urethra, verumontanum, or seminal vesicle; in females, it may open into the urethra, vestibule, vagina, etc. This indicates that the ureter connected to the upper kidney must traverse a longer distance. The Weigert-Meyer law describes this relationship. It appears that the lower kidney is the normal one, while the upper kidney is an abnormal or superfluous kidney. There are further reasons supporting this observation: the upper kidney often has an abnormal morphology and is frequently associated with complications such as hydronephrosis, stones, or subcutaneous nodules. Statistics show that about 50% of cases involve complications, and its function is often abnormal. In contrast, the lower kidney meets the criteria of a normal kidney in both morphology and function (Figures 1, 2).
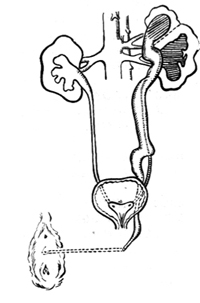
Figure 1 Ureteral malformation

Figure 2 Ectopic ureteral orifice
Patient: Dang ××, female, 17 years old, hospitalization number: 10785
bubble_chart Clinical Manifestations

2. Duplex kidney with complications, presenting symptoms such as pyelitis, kidney stones, subcutaneous nodules, tumors, hydronephrosis, etc., and discovered during a comprehensive urological examination.
3. Complete duplication of the ureter, with the ureter opening into the vestibule, vagina, etc. This results in a history of enuresis from childhood, with bedwetting at night and frequently damp underwear during the day, while the patient still has normal urination. With such a history, careful examination of the vulva often reveals an abnormal ureteral orifice. Even if the abnormal ureteral opening cannot be found, intravenous pyelography can usually confirm this congenital anomaly.
Pyelography is particularly important. Whenever possible, perform retrograde pyelography by catheterization for clear imaging. If catheterization is restricted and the examination is unsatisfactory, switch to intravenous pyelography. If the upper renal segment fails to visualize due to renal function but remains highly suspicious, use double-contrast agents and delayed imaging to ensure clear visualization for accurate diagnosis.
bubble_chart Treatment Measures
1. For the first scenario mentioned above, no special treatment is required.
2. For the second scenario, due to the presence of significant complications, an upper renal segmentectomy (the renal segment with complications) is performed. This type of surgery is much easier to handle than a standard partial nephrectomy because it has its own independent blood supply.
Pyelonephritis; kidney stones; subcutaneous node; tumor; hydrops


