| disease | Zygomatic Fracture |
| alias | Fracture of Zygoma |
The zygomatic bone and zygomatic arch are relatively prominent parts of the face and are prone to fractures upon impact. The zygomatic bone connects with the maxilla, frontal bone, sphenoid bone, and temporal bone, with the largest connecting surface being with the maxilla. Therefore, fractures of the zygomatic bone (fracture of malar bone) are often accompanied by fractures of the maxilla. The temporal process of the zygomatic bone connects with the zygomatic process of the temporal bone to form the zygomatic arch, which is narrower and more susceptible to fractures (fracture of zygomatic arch).
bubble_chart Clinical Manifestations
It can generally be divided into zygomatic fracture, zygomatic arch fracture, combined zygomatic-zygomatic arch medial malleolus fracture, and complex zygomatic-maxillary fracture. Zygomatic arch fractures can further be classified into bifocal and trifocal fractures. Knight and North proposed a six-type classification system: ① Non-displaced fracture; ② Zygomatic arch fracture; ③ Zygomatic body fracture displaced inward and downward without rotation; ④ Medially rotated zygomatic body fracture, with counterclockwise rotation on the left side, clockwise rotation on the right side, or rotation toward the midline. X-ray shows the infraorbital rim displaced downward and the zygomaticofrontal process displaced medially; ⑤ Laterally rotated zygomatic body fracture, with clockwise rotation on the left side, counterclockwise rotation on the right side, or rotation away from the midline. X-ray shows the infraorbital rim displaced upward and the zygomaticofrontal process displaced laterally; ⑥ Complex fracture. They suggested that types ② and ⑤ fractures are stable after reduction and do not require fixation, while types ③, ④, and ⑥ fractures are unstable after reduction and require fixation.
1. Depression of the zygomatic region The displacement direction of fractured fragments in zygomatic and zygomatic arch fractures mainly depends on the direction of the external force, often resulting in inward displacement (Figure 1). In the early stages post-injury, depression of the zygomatic region may be observed. However, due to local swelling, the depression deformity may not be obvious and can be mistaken for simple soft tissue injury. After several days, when the swelling subsides, local depression reappears.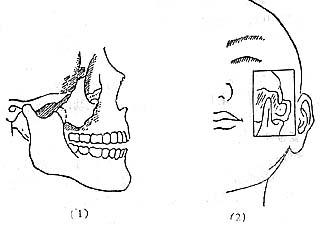
Figure 1 Displacement in zygomatic and zygomatic arch fractures (1) Downward and backward displacement after zygomatic fracture (2) Inward displacement in zygomatic arch fracture.
2. Restricted mouth opening Due to inward displacement of fractured fragments, the temporalis and masseter muscles are compressed, hindering coronoid process movement, leading to pain and restricted mouth opening (Figure 2).
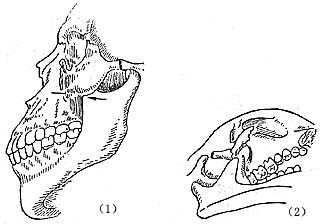
Figure 2 Inward displacement of zygomatic and zygomatic arch fractures restricting mouth opening (1) Zygomatic displacement compressing the coronoid process (2) Zygomatic arch inward displacement obstructing coronoid process movement
3. Diplopia The zygomatic bone forms most of the lateral orbital wall and infraorbital rim. After zygomatic fracture displacement, diplopia may occur due to eyeball displacement, extraocular muscle hemorrhage, local edema, or entrapment of the torn inferior oblique muscle in the fracture line, restricting eye movement.
4. Ecchymosis In cases of closed zygomatic orbital wall fractures, hemorrhagic ecchymosis may appear in the periorbital subcutaneous tissue, eyelids, and subconjunctival area.
5. Neurological symptoms Fractures of the zygomaticomaxillary process may injure the infraorbital nerve, causing numbness in the nerve's distribution area. If the zygomatic branch of the facial nerve is also injured during the fracture, incomplete eyelid closure may occur.
The diagnosis of zygomatic arch fracture can be confirmed based on the history of injury, clinical features, and X-ray examination.
Palpation of the fracture site may reveal tenderness, depression, or displacement, with possible step formation at the zygomaticofrontal suture, zygomaticomaxillary suture, and infraorbital rim. If palpation is performed intraorally along the vestibular groove in a posterior-superior direction, the reduction of space between the zygomatic bone and the maxilla or coronoid process can be assessed. These findings all contribute to the diagnosis of zygomatic fracture.
X-ray examination typically includes the naso-chin view and the zygomatic arch view. The naso-chin view not only reveals the fracture of the zygomatic bone and arch but also allows observation of any abnormalities in the orbital, maxillary sinus, and infraorbital foramen structures. The zygomatic arch view clearly displays the fracture and displacement of the zygomatic arch.
bubble_chart Treatment Measures
If there is only grade I displacement after a zygomatic or zygomatic arch fracture, with no obvious deformity and no functional impairments such as limited mouth opening or diplopia, surgical treatment may not be necessary. However, reduction surgery should be performed in all cases with limited mouth opening. Even in the absence of functional impairment, surgical reduction may be considered if significant deformity is present.



