| disease | Congenital Radial Head Dislocation |
Congenital radial head dislocation is rare, with McFarland first reporting 11 cases in 1936, and to date, fewer than 100 cases have been documented in the literature.
bubble_chart Etiology
The cause of the disease remains unclear. The radial head dislocation can be anterior, posterior, or lateral (Figure 1)
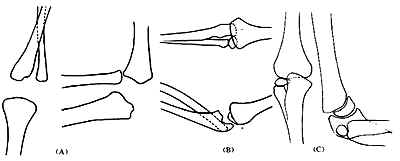
(A) Anterior radial head dislocation (B) Posterior radial head dislocation (C) Posterolateral radial head dislocation
bubble_chart Pathological Changes
Good and Wicks proposed that this disease is a developmental radial head dislocation with no history of trauma, backward bending of the proximal ulna, and involvement of the radial head epiphyseal plate.
bubble_chart Clinical Manifestations
Asymmetry in both elbows, sometimes accompanied by clicking or limited movement during extension or flexion of the elbow joint. The direction of ulnar curvature is related to the type of dislocation. For example, in anterior dislocation of the radial head, the ulna protrudes forward; in posterior dislocation of the radial head, the ulna protrudes backward; and in lateral dislocation, the ulna protrudes outward. When anterior dislocation of the radial head occurs, the range of elbow flexion decreases, and the dislocated radial head can be palpated in the cubital fossa. When posterior dislocation of the radial head occurs, the elbow joint cannot fully extend, and the protruding radial head can be palpated at the Zhouhou Fang. X-ray images show that, on the lateral view of the elbow joint, the longitudinal axis of the radial shaft does not intersect with the humeral head. The radial head appears dome-shaped, and the radial neck articulates with the humeral capitulum, where indentations may occur at the contact area.
bubble_chart DiagnosisNo history of trauma, the dislocated radial head can be palpated at the elbow, and X-ray shows radial head dislocation, confirming the diagnosis.
bubble_chart Treatment Measures
1. Non-surgical therapy For radial head dislocation in infants and young children, closed reduction may be attempted. For posterior dislocation of the radial head, the forearm should be fixed in supination and the elbow joint in extension; for anterior dislocation, the elbow joint should be fixed in flexion. After reduction, gypsum fixation is maintained for 4-6 weeks. However, the results are often disappointing.
2. Surgical treatment For children aged 3 years or older, open reduction of the radial head is performed, along with shortening osteotomy at the midpoint of the radial shaft where the pronator teres attaches, and annular ligament reconstruction. A Kirschner wire is temporarily used to fix the radial head to the capitellum. A posterior elbow splint with gypsum is applied for 6 weeks, after which the Kirschner wire is removed, and elbow joint mobility exercises are initiated. An elbow brace is used for three months.
For older children with radial head dislocation where reduction is not possible, radial head resection may be considered during adolescence.
It should be differentiated from traumatic radial head dislocation. Common conditions include Monteggia fracture, radial neck fracture, pulled elbow, and other injuries causing traumatic radial head dislocation. Ulnar bowing is not exclusive to congenital radial head dislocation and can occur in unreduced traumatic radial head dislocation. In congenital radial head dislocation, the capitellum is small, and the radial head is oval-shaped. Ossification of the soft tissues around the radial head suggests an unreduced traumatic radial head dislocation.



