| disease | Vitamin C Deficiency Disease |
| alias | Scurvy, Scurvy |
Scurvy is a systemic disease caused by a prolonged deficiency of vitamin C (ascorbic acid). It is relatively uncommon nowadays, but still occurs in northern pastoral areas lacking fresh vegetables and fruits, as well as in urban and rural areas where artificially fed infants are neglected in terms of complementary food supplementation, particularly in remote rural regions due to improper feeding practices.
bubble_chart Etiology
1. Inadequate intake: If the mother's nutrition is adequate, the infant has appropriate vitamin C reserves at birth. The umbilical bleeding plasma vitamin C level is 2-4 times higher than that of maternal plasma, so scurvy is less common in infants under 3 months. However, if the mother's diet lacks vitamin C, the newborn may also develop scurvy. Normal human milk contains about 40-70 mg/L (4-7 mg/dl) of vitamin C, which can meet the needs of most infants. The vitamin C content in breast milk is directly proportional to the mother's dietary intake of vitamin C. If the mother's diet is deficient in vitamin C, her breastfed infant may develop scurvy. Fresh animal milk contains less vitamin C than human milk, with cow's milk generally having only 1/4 the amount of human milk. After storage, sterilization, and dilution, very little remains. Therefore, infants fed with cow's milk, lance asiabell root, or non-fortified milk powder, rice cakes, flour paste, etc., are highly susceptible to scurvy if vitamin C, fruits, or vegetables are not supplemented in a timely manner. Scurvy in older children is caused by a lack of fresh vegetables and fruits in their diet.
2. Increased demand: When the metabolic rate increases, the need for vitamin C rises. During periods of active growth, the vitamin C content in body tissues decreases sharply. Premature labor infants grow and develop faster, requiring relatively more vitamin C than normal infants, and thus need additional supplementation. During febrile sexually transmitted diseases, acute or chronic infectious diseases such as diarrhea, dysentery, pneumonia, subcutaneous node, etc., the demand for vitamin C increases. If the illness lasts for an extended period without increased vitamin C intake, varying degrees of scurvy may develop.
3. Other factors: Long-term intake of large amounts of vitamin C increases its catabolism and renal excretion, lowering plasma vitamin C levels. If high doses of vitamin C are suddenly discontinued, scurvy may occur. If large amounts of vitamin C are used during pregnancy, the newborn may still develop scurvy even if given the conventional daily dose of vitamin C after birth.Vitamin C is essential for the formation of normal collagen tissue in the human body. The human body cannot synthesize vitamin C and must obtain it through diet. Vitamin C is widely found in fruits and vegetables. Fruits such as citrus, grapes, and berries are rich in vitamin C, while vegetables like leafy greens, sprouted vegetables or legumes, tubers, and potatoes also contain significant amounts. The adrenal glands and the lens of the eye have particularly high concentrations of vitamin C. Vitamin C is highly soluble in water and has strong reducing properties. It is easily destroyed under the following conditions: ① alkaline environments; ② trace amounts of copper; ③ the release of ascorbic acid oxidase when vegetables are chopped, cut, crushed, or torn; ④ prolonged boiling or heating; ⑤ prepared dishes left standing for too long.
The structure of vitamin C resembles that of a monosaccharide. It is widely recognized as an essential cofactor for the enzymes prolyl hydroxylase and lysyl hydroxylase, which are necessary for collagen biosynthesis, and it enhances the activity of various hydroxylases and oxidases. Due to its reversible oxidation-reduction capability, it plays an active role in microsomal electron transport. It is crucial for preventing collagen depolymerization and maintaining the integrity of the extracellular matrix. In the body, it facilitates the conversion of folic acid to tetrahydrofolic acid, promoting red blood cell maturation. It also reduces ferric iron to ferrous iron, aiding intestinal iron absorption, hemoglobin synthesis, and the storage of ferritin in the liver. Additionally, it promotes the synthesis of certain adrenal and pituitary hormones, immunoglobulins, neurotransmitters, and common bletilla tuber.
Vitamin C deficiency can lead to impaired collagen fiber formation, reduced intercellular matrix, stagnation in dentin and osteoid tissue formation, capillary bleeding, delayed wound healing, and disorders in folic acid and iron metabolism, resulting in anemia and a series of other pathological changes.
bubble_chart Pathological Changes
The main lesions are caused by a deficiency of collagen, leading to bleeding and skeletal changes. When vitamin C is deficient, the primary components of collagen—hydroxyproline and chondroitin sulfate—decrease, impairing the formation of collagen fibers. As a result, the following pathological changes may occur: ① Due to impaired connective tissue formation, the lack of binding material between capillary endothelial cells increases capillary fragility and vascular permeability, leading to bleeding in the skin, mucous membranes, subperiosteal areas, joint cavities, and muscles. ② Skeletal lesions: These often occur at the costochondral junctions and the ends of long bones, particularly near the wrists, knees, and ankles. Since matrix formation is affected, osteoblasts can no longer produce normal intercellular osteoid tissue, and endochondral ossification is impaired. However, calcium deposition in the cartilage matrix continues. A characteristic feature is the accumulation of calcium in the metaphyseal provisional calcification zone, forming a dense and thickened band. Osteogenesis is inhibited, preventing the formation of bone tissue. Existing trabeculae become brittle and prone to fracture, and the metaphyseal bone becomes fragile, often leading to fractures and epiphyseal separation. The original cortical and cancellous bones undergo generalized atrophy due to internal resorption. The periosteum loosens, and subperiosteal hemorrhage is common due to bleeding tendencies. ③ Dental lesions: Gingival congestion and edema, or degeneration of the odontoblastic layer, cause loose teeth due to collagen deficiency. Gingival lesions begin with hyperplasia of the gingival papillae and granulation tissue growth, followed by gradual necrosis. This condition is commonly seen in children who have already erupted teeth. In severe cases, skeletal muscle degeneration, cardiac hypertrophy, bone marrow suppression, and adrenal atrophy may occur.

The disease can occur at any age, but is most commonly seen in children aged 6 to 24 months.
1. Systemic Symptoms The onset is gradual, taking about 4 to 7 months from dietary vitamin C deficiency to the development of scurvy. Early non-specific symptoms often include irritability, weakness, fatigue, loss of appetite, weight loss, and pallor. Digestive disturbances such as vomiting and diarrhea may also occur, often unnoticed by parents. This stage may be referred to as the latent phase.
Low-grade fever is generally present, likely related to hemorrhage. With complications, the temperature may rise further. The pulse increases proportionally with the temperature, possibly due to sympathetic nerve excitation caused by leg pain. Breathing may also be shallow, likely due to rib pain.
2. Local Symptoms Swelling and pain in the lower limbs, especially the calves, are most common. Swelling typically occurs along the tibial shaft, with significant tenderness. The local temperature may be slightly elevated but without redness. In later stages, the affected limbs often assume a fixed position: legs abducted, calves bent inward like a frog, unwilling to move, presenting as pseudoparalysis. Due to severe pain, the child fears any contact with the legs and may cry when approached. The swelling is caused by subperiosteal hemorrhage and does not pit upon finger pressure.
Sharp protrusions may form at the junctions of the ribs and costal cartilages, known as scorbutic beads. A depression can be felt on the inner side of the protrusion, caused by partial dislocation of the sternal plate at the rib-cartilage junction. In contrast, rickets beads result from widening of the epiphyseal cartilage and are symmetrically prominent on both sides without such depressions.
3. Hemorrhagic Symptoms Bleeding of varying sizes and severity can occur anywhere in the body, most commonly subperiosteal hemorrhages in long bones, especially the distal femur and proximal tibia. These hemorrhages may not be easily detected by X-ray until the healing phase, when surface calcification begins. Petechiae and ecchymoses are often seen near skeletal lesions, particularly around the knees and ankles. Petechiae may also appear elsewhere. Submucosal bleeding in the gums is common, mostly seen during teething or after teeth have erupted, most prominently in the upper incisor area but also around emerging molars or incisors. The gums appear purplish-red, swollen, smooth, and friable, bleeding easily with slight pressure. If swelling expands, it may cover the teeth, with surface static blood accumulation. Secondary Vincent's infection can lead to local necrosis, foul odor, and tooth loss. Eyelid or conjunctival bleeding may cause a bluish-purple appearance. Subperiosteal hemorrhage in the orbit may cause exophthalmos. In advanced stages, gastrointestinal, genitourinary, or meningeal bleeding may rarely occur. About one-third of patients have red blood cells in their urine, but gross hematuria is seldom observed.
Additionally, older children with scurvy may exhibit follicular hyperkeratosis of the skin, which is difficult to distinguish from that caused by vitamin A deficiency. Infant patients often have megaloblastic anemia due to impaired folate metabolism, possibly combined with folate deficiency. Impaired iron absorption and utilization may also lead to concurrent iron-deficiency anemia.
Typical scurvy presents with obvious symptoms, making diagnosis relatively easy. However, latent and early-stage scurvy lacks specific symptoms, making diagnosis more challenging and requiring a comprehensive analysis that includes feeding history and other examinations.
1. Feeding history and clinical symptoms: Formula-fed infants without vitamin C supplementation, or breastfeeding mothers lacking fresh vegetables or fruits in their diet, or mothers who habitually consume only pickled vegetables. The peak age for scurvy (3–18 months), combined with the aforementioned nonspecific symptoms and feeding history, can provide clues for early diagnosis. If the disease has progressed to a certain stage or advanced stage, diagnosis can be based on symptoms such as limb swelling and pain, frog-leg posture, and bleeding under the gums and mucous membranes.
2. X-ray examination: X-ray examination of the long bones in the limbs is extremely important for diagnosing this disease. X-rays taken of the knees, ankles, and wrists can provide evidence for early diagnosis of scurvy, particularly the slightly thickened and irregular white epiphyseal line (indicating thickening of the provisional calcification zone due to calcium accumulation), a full-width black line or black dots at the lateral angles below the epiphyseal line near the diaphysis, or a triangular defect (indicating varying degrees of bone rarefaction, appearing as translucent lines or dots on the X-ray), which are characteristic of this disease.
As the disease progresses, the following changes may be observed: ① Thinning of the bone cortex and atrophy of the trabecular structure, leading to increased transparency of the diaphysis, resembling ground glass; ② The aforementioned rarefied dots or lines enlarge, forming a full-width black band, which may be referred to as the "scurvy zone"; ③ The center of the ossified epiphysis also appears ground-glass-like, surrounded by a distinct white ring, densest near the metaphysis; ④ Small bone spurs appear at the junction of the epiphyseal line and the thickened epiphyseal line on both sides of the epiphysis, extending laterally, hence termed "lateral spurs"; ⑤ Shadows from subperiosteal hemorrhages give the affected long bones a club-shaped or spindle-shaped appearance, sometimes forming a dumbbell shape if hemorrhages occur at both distal ends of the long bone, with clearer outlines after treatment (Figure 1); ⑥ In severe cases, separation and displacement of the epiphysis and diaphysis may occur; ⑦ The anterior ends of the ribs widen, with rounded protrusions resembling a tongue depressor, easily distinguishable from the cup-shaped ends of rickets.
|
|
|
(1) | (2) |
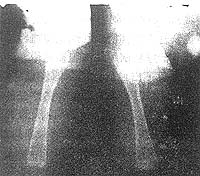

Figure 1 X-ray of long bones in scurvy, showing subperiosteal hematoma
A 7-month-old boy, (1) Spindle-shaped swelling and density of the thigh soft tissue, indicating massive subperiosteal hemorrhage; (2) Taken 24 days after treatment, showing significant improvement in bone rarefaction, thickened provisional calcification zone, disappearance of the translucent zone, and subperiosteal hematoma with substantial calcium deposition.
3. Laboratory Findings Laboratory tests are far less straightforward than X-ray examinations in diagnosing scurvy. ① Fasting plasma vitamin C concentration >6 mg/L (0.6 mg/dL) can rule out scurvy. However, lower concentrations do not confirm the presence of scurvy, as clinical diagnosis often does not correlate with plasma vitamin C levels. Specimens must be tested within 48 hours of collection. ② Measuring the ascorbic acid concentration in the leukocyte-platelet layer (buffy coat) obtained by centrifuging oxalate-treated blood is a better method for confirming vitamin C deficiency. The normal range is 280–300 mg/L (28–30 mg/dL). A drop to zero indicates latent scurvy, even in the absence of clinical symptoms. ③ Another effective method is the tolerance test, where a 4% solution of ascorbic acid (20 mg/kg in saline) is administered intravenously. If the urine sample contains >15 mg/L (1.5 mg/dL) of vitamin C after 4 hours, scurvy can be excluded. ④ In vitamin C deficiency, 24-hour urinary vitamin C excretion decreases (normal range: 20–40 mg). Even with high-dose supplementation, urinary vitamin C may not return to normal levels initially, as the body prioritizes replenishing tissues. Excess vitamin C is excreted only after tissues are saturated and blood levels rise. ⑤ Additionally, nonspecific aminoaciduria is observed in scurvy, though blood amino acid levels remain normal. Tyrosine loading tests show that scurvy infants excrete metabolites similar to those of premature infants. Capillary fragility tests may be negative in latent scurvy but positive in overt scurvy. Serum calcium and phosphorus levels are normal, while alkaline phosphatase activity is reduced, contrasting with active rickets. In advanced stages, significant anemia (usually microcytic) is common, though macrocytic anemia may occur if folate metabolism is impaired.
4. Therapeutic Trial Scurvy responds specifically to vitamin C treatment, which can aid in diagnosis.
bubble_chart Treatment Measures
For mild cases, administer vitamin C orally, 100–150 mg three times daily. For severe cases and those with symptoms such as vomiting, diarrhea, or visceral bleeding, switch to intravenous injection, administering the full daily dose at once. Additionally, provide fresh orange juice and other foods rich in vitamin C. Furthermore, supplement other vitamins as needed, with particular attention to addressing concurrent vitamin D deficiency. For patients with combined megaloblastic anemia, increase the therapeutic dose of vitamin C and administer an appropriate amount of folic acid.
Children with significant bone lesions should rest and minimize movement to prevent fractures and epiphyseal dislocation. For those with gum bleeding, maintain oral hygiene.
For patients with complications, provide appropriate treatment targeting the disease cause and symptoms.
With the above treatment, mild cases generally experience relief from local pain and tenderness within 1-2 days, improved appetite, and the ability to move limbs in about 4-5 days. Symptoms disappear within 7-10 days, body weight gradually increases, and local tenderness completely subsides within approximately 3 weeks. Meanwhile, capillary fragility also returns to normal. Megaloblastic anemia shows a significant increase in reticulocytes after treatment with vitamin C and folic acid. Recovery from bone lesions and hematomas caused by submembrane bleeding takes longer, with severe cases requiring several months to resolve. Even severe bone lesions can recover easily without causing deformities. However, if left untreated, children with scurvy may die from complications such as malnutrition, hemorrhage, or infection.
The high vitamin C content in breast milk is one of the reasons to emphasize breastfeeding. The diet of pregnant and lactating women should include foods rich in vitamin C, such as fresh vegetables and fruits, or vitamin C tablets dissolved in water with sugar for oral intake. The recommended daily intake of vitamin C is approximately 80–100 mg or more to ensure that the fetus and infant receive sufficient ascorbic acid. Zhu Futang (1936) conducted an experiment showing that consuming 0.5 kg each of Chinese cabbage and white radish daily could increase the vitamin C concentration in breast milk to as high as 60 mg/L (6 mg/dl).
Newborns should be supplemented with vitamin C-rich and easily digestible foods, such as freshly squeezed orange juice, tomato juice, cabbage soup, or radish juice, starting at 2–4 weeks after birth. By 4–5 months, mashed vegetables can be introduced. Artificially fed infants should receive an appropriate daily supplement of vitamin C. The recommended daily intake for normal infants is 30 mg, toddlers 30–35 mg, older children 40–60 mg, and premature infants 100 mg, as recommended by the Chinese Nutrition Society in 1988. During illness, when vitamin C consumption increases, a higher dose should be administered.
This disease can coexist with rickets and malnutrition. When complicated by rickets, the X-ray images may show the different manifestations of both conditions, leading to confusion. Children with scurvy have reduced resistance and often develop complications such as otitis media, furunculosis, pneumonia, and other infections.
A thorough differential diagnosis should be conducted to avoid delaying effective treatment due to a misdiagnosis of fistula disease or performing unnecessary surgical procedures by mistakenly identifying it as localized inflammation.
1. Limb swelling and pain: It should be differentiated from suppurative arthritis, osteomyelitis, cellulitis, and deep abscesses. These conditions are more common in unilateral limbs and are accompanied by localized redness, swelling, and heat, with significant systemic symptoms such as high fever, toxic manifestations, and increased white blood cells, all of which are distinctly different from scurvy. Wind-dampness arthritis is rare in infants under 2–3 years old, is migratory, and has other specific symptoms and signs of wind-dampness heat that aid in differentiation.
Subperiosteal hemorrhage in scurvy sometimes needs to be differentiated from tumors, but other symptoms of scurvy make it easily distinguishable from tumors. If necessary, X-ray examination and therapeutic trials can clarify the diagnosis.
The systemic symptoms and bone tenderness in infantile cortical hyperostosis may sometimes resemble scurvy, but the lesions are more common in flat bones such as the mandible, scapula, calvaria, and clavicle. The face is often affected, and sometimes the limbs are involved as well. Increased erythrocyte sedimentation rate and elevated serum alkaline phosphatase levels aid in differentiation. The onset age is typically within the first 6 months of life, whereas scurvy usually occurs after 6 months. The course of infantile cortical hyperostosis is irregular, ranging from weeks to months, sometimes with recurrent episodes, but it generally resolves naturally. X-ray findings show bone hyperplasia and thickened cortex, which gradually resolve over months, with no overlap with scurvy.
The onset age of acrodynia differs from scurvy, and it is characterized by distinctive redness, itching, and severe pain in the hands and feet, hypertension, sweating, and photophobia. In severe cases, fingers and toes may turn black or even detach, making it easily distinguishable from scurvy (refer to the section on mercury poisoning in the toxicology chapter).
2. Pseudoparalysis of limbs: It should be differentiated from poliomyelitis, rickets, trauma, and congenital syphilis: ① Poliomyelitis presents as flaccid paralysis without swelling or pain, along with other systemic symptoms, making it distinctly different from scurvy; ② Rickets has specific signs and X-ray findings; ③ Traumatic cases should have a history of injury, and bilateral symmetrical injuries are extremely rare. X-ray examination reveals significant differences; ④ Congenital syphilis mostly occurs in infants under 4 months old, with mothers having overt or latent syphilis. The infant exhibits specific signs of congenital syphilis, and serological tests and long bone X-rays can aid in differentiation.
3. Hemorrhagic symptoms: They should be differentiated from other bleeding disorders: ① Thrombocytopenic purpura, allergic purpura, and hemophilia can be distinguished based on platelet counts, bleeding and clotting times, other coagulation tests, and family history; ② Hemorrhage in leukemia is accompanied by characteristic changes in blood and bone marrow morphology; ③ Septicemic epidemic cerebrospinal meningitis presents with neurological signs and cerebrospinal fluid changes, and causative bacteria can be easily identified from skin purpura or cerebrospinal fluid, making differentiation straightforward; ④ Orbital hemorrhage and exophthalmos should be differentiated from neuroblastoma and chronic xanthoma, as the latter two lack other features of scurvy; ⑤ Gum bleeding should be differentiated from gingivitis, which is rare in infants and typically presents with reddened gums without other scurvy symptoms.


