| disease | Temporal Bone Fracture |
Temporal bone fractures are part of skull base fractures, with the petrous portion being the most commonly fractured among the petrous, squamous, and mastoid parts. This is because the petrous portion contains various foramina, canals, and air cells, making it more fragile. As a result, one-third of skull base fractures occur here.
bubble_chart Clinical Manifestations
Based on the relationship between the fracture and the long axis of the petrous bone, it can be divided into three types: longitudinal fracture, transverse fracture, and mixed-type fracture (Figure 1). Longitudinal fractures are the most common, accounting for approximately 70–80%. The fracture line runs parallel to the long axis of the petrous bone, extending from the mastoid antrum to the roof of the Eustachian tube, primarily damaging the middle ear and rarely affecting the labyrinth. Transverse fractures account for about 20%, with the fracture line crossing the long axis of the petrous bone, often passing through the jugular fossa and internal auditory canal, traversing the inner ear labyrinth, and less frequently injuring the middle ear. Mixed-type fractures mostly occur due to compressive trauma to the skull, with multidirectional fracture lines, often involving the external ear, inner ear, or middle ear, and are associated with severe cranial injuries.
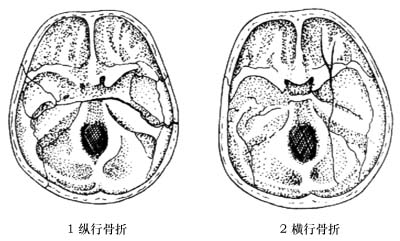
Figure 1 Temporal bone fracture
It can cause ear bleeding, external auditory canal injury, tympanic membrane rupture, cerebrospinal fluid fistula disease, deviation of the mouth, hearing loss, tinnitus, vertigo, eye tremor, nausea, vomiting, etc. However, due to frequent concurrent closed or open craniocerebral trauma, the symptoms are complex and complications vary. The prognosis depends on the extent and severity of the fracture, with longitudinal fractures generally having a better prognosis.
bubble_chart Treatment MeasuresFirst, manage according to neurosurgical principles: bed rest, anti-shock measures, and intravenous administration of intracranial pressure-lowering medications. For tympanic membrane injuries, use dry treatment and avoid ear drops or irrigation. In cases of cerebrospinal fluid otorrhea, avoid ear canal blockage. Administer high-dose antibiotics to prevent intracranial infection; for cases that do not heal over time, perform meningeal repair surgery once the condition improves. If acute suppurative otitis media occurs in the affected ear, consider a mastoidectomy to establish external drainage. Provide sedatives for patients with vestibular symptoms. For cases of facial deviation, consider facial nerve exploration after the condition stabilizes. For conductive deafness alone, consider traumatic ossicular chain disruption, and perform tympanoplasty later to improve hearing.
The differential diagnosis between longitudinal fracture and transverse fracture is shown in Table 1
Table 1 Differential Diagnosis Table of Petrous Bone Fracture
| Longitudinal fracture | Transverse fracture | |
| Ear bleeding | Very common | Rare |
| External auditory canal injury | Occasionally occurs | None |
| Tympanic membrane rupture | Very common | Rare, hemotympanum more common |
| Cerebrospinal fluid fistula disease | Occasionally occurs | Occasionally occurs |
| Deviation of mouth | Occurs in 25% of injured, often temporary | Occurs in 50% of injured, often permanent |
| Hearing loss | Mixed type, partial recovery possible | Grade III sensorineural, no hope of recovery |
| Vertigo | Occasionally occurs, mild and mostly temporary | Often occurs, more severe, lasts longer |
| Nystagmus | Mild or none | Nystagmus towards healthy side, lasts about 2-6 weeks |
| Vestibular function | Normal or grade I decline | Absent |
| X-ray or CT scan | Fracture line may be seen in squamous or mastoid part of temporal bone, longitudinal in petrous part | 50% of injured show transverse fracture line in petrous part of temporal bone |



