| disease | Infratemporal Space Infection |
Infratemporal space infection refers to an acute suppurative infection in the infratemporal space. The main clinical manifestations include swelling above and below the zygomatic arch and behind the mandibular ramus, deep tenderness, and varying degrees of restricted mouth opening.
bubble_chart Etiology
The infratemporal space is located below the temporal bone. Its anterior boundary is the posterior aspect of the maxillary tuberosity and the zygomatic process of the maxilla; the posterior boundary is the styloid process and the styloid muscles; the medial boundary is the lateral surface of the lateral pterygoid plate of the sphenoid bone; the lateral boundary is the upper part of the mandibular ramus and the zygomatic arch; the superior boundary is the infratemporal surface of the greater wing of the sphenoid bone and the infratemporal crest; the inferior boundary is the plane of the lower edge of the lateral pterygoid muscle, which separates it from the pterygomandibular space. Within this space, the adipose tissue, internal maxillary artery and vein, pterygoid venous plexus, and branches of the mandibular and maxillary divisions of the trigeminal nerve communicate with the temporal, pterygomandibular, parapharyngeal, buccal, and pterygopalatine spaces. It also connects with the intraorbital and intracranial regions via the inferior orbital fissure, foramen ovale, and foramen spinosum (Figure 1).
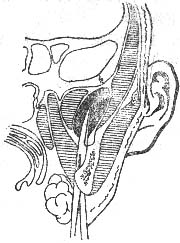
Figure 1 Anatomical location of the infratemporal space and the submandibular approach for external incision and drainage.
Infection can spread from adjacent spaces, such as the pterygomandibular space, or be introduced during anesthesia blockade of the maxillary tuberosity, foramen ovale, or foramen rotundum. It may also arise from periapical infections of maxillary molars or post-extraction infections.
bubble_chart Clinical ManifestationsThe infratemporal space is deep and concealed. When infection occurs, external manifestations are often subtle. Careful examination may reveal slight swelling above and below the zygomatic arch and behind the mandibular ramus, with deep tenderness and varying degrees of restricted mouth opening. However, infections in the infratemporal space often involve adjacent spaces, leading to swelling in the temporal region, masseteric region, buccal area, and the maxillary tuberosity area inside the mouth, along with corresponding symptoms of the associated space infections.
1. Medical History Prior to infratemporal space infection, there may be a history of pericoronitis or periapical periodontitis of the maxillary third molar. Additionally, histories such as posterior superior alveolar nerve block anesthesia, foramen ovale anesthesia, and infratemporal-trigeminal-sympathetic nerve block should not be overlooked.
2. Clinical Manifestations Due to the deep and concealed anatomical location of the abscess, although systemic symptoms of infection and toxicity such as high fever, headache, loss of appetite, and elevated white blood cell count are prominent, facial redness and swelling are not very noticeable. Instead, indirect manifestations include significant redness and swelling at the mucosal fold of the maxillary tubercle on the affected side, swelling and shallowing or bulging of the vestibular sulcus, obvious tenderness, and fluctuation. Pus can be easily aspirated by puncture at this site. Swelling and tenderness are also present above and below the zygomatic arch and in the upper posterior mandibular region.
Active application of high-dose antibiotics should be employed for treatment. If symptom relief is not evident and pus is detected through intraoral (lateral to the maxillary tuberosity) or extraoral (between the zygomatic arch and sigmoid notch) puncture, prompt incision and drainage should be performed.
The incision and drainage can be performed via intraoral or extraoral routes. The intraoral approach involves an incision at the lateral maxillary tuberosity in the vestibular mucosal fold, followed by separation toward the posterior superior direction along the medial side of the coronoid process of the mandibular ramus using a hemostat to reach the abscess cavity. The extraoral approach typically involves a curved incision below the mandibular angle. After transecting the platysma muscle, entry into the abscess cavity is achieved between the posterior border of the mandibular ramus and the medial pterygoid plate.



