| disease | Fracture of the Radial Neck |
Fractures of the cervical vertebra of the radius are relatively rare and are often associated with radius head fractures, but they can also occur alone. The injury mechanisms and diagnostic and treatment requirements for both are similar.
bubble_chart Pathogenesis
The carrying angle and elbow joint typically exhibit a natural outward tilt. When falling and landing on the hand, the force travels from the distal to the proximal end along the radius toward the elbow. Upon reaching the upper end of the radius, the radial head collides with the humeral capitulum, resulting in a fracture of the radial head, radial neck, or both. If the force persists, it may also lead to fractures of the olecranon or humerus external condyle, as well as dislocation.
bubble_chart Clinical Manifestations
1. Pain: There is obvious pain, tenderness, and forearm rotation pain at the radial head.
2. Swelling: It is generally milder than typical fractures and mostly limited to the radial head.
3. Restricted rotation: In addition to affecting elbow flexion and extension, the main manifestation is significant impairment in forearm placement movement.
4. Others: Attention should be paid to possible injury to the deep branch of the radial nerve.
In addition to trauma history and clinical symptoms, the diagnosis and classification are primarily based on X-ray plain films. Analyzing the imaging findings, it is generally divided into the following four types (Figure 1).
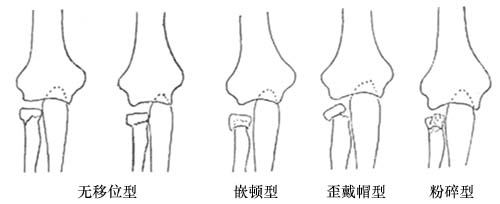
Figure 1 Schematic diagram of the classification of radial cervical vertebra fractures
1. Non-displaced type: Refers to fissures or greenstick fractures in the radial neck. This type is stable and usually does not require reduction. It is more common in children.
2. Impacted type: Mostly occurs when the distal fragment of the radial cervical vertebra fracture is impacted into the proximal fragment. This type is also relatively stable.3. Tilted cap type: Refers to the fracture fragment of the radial head tilting to one side after a radial cervical vertebra fracture, resembling the posture of a person wearing a French cap.
4. Comminuted type: Refers to fractures of the radius, neck, and/or head that are broken into three or more fragments.
bubble_chart Treatment Measures
1. Non-displaced and embedded type: Only the elbow joint is immobilized with an upper limb gypsum splint or gypsum in functional position for 3 to 4 weeks.
2. Displaced type: First, perform manual reduction. Under local anesthesia, the surgeon places one thumb on the radial head while holding the patient's wrist with the other hand. With slight traction, quickly rotate the wrist inward and outward several times, which usually achieves reduction. If reduction is unsatisfactory, open reduction of the radial head may be performed, and if necessary, a seasonal epidemic screw internal fixation procedure (Figure 2). For unstable and comminuted types, radial head resection is required, but the epiphyseal block must not be removed in cases of epiphyseal injury.
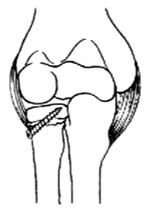
Figure 2 Schematic diagram of open reduction and screw (internal fixation) for radial cervical vertebra fracture.
The condition is generally good. In individual cases, such as late-stage (third-stage) injuries with symptoms of humeroradial joint inflammation, radial head resection may be performed. Additionally, a few cases may lead to premature epiphyseal closure, epiphyseal necrosis, or proximal radioulnar joint fusion. The first two have little impact on elbow function, while the latter, caused by improper surgical technique, should be prevented.


