| disease | Congenital Abduction Contracture of the Hip |
This disease is a postural deformity, primarily characterized by unequal leg lengths. Although it has a high incidence rate, it is often overlooked by parents, resulting in few medical consultations.
bubble_chart Pathogenesis
It is generally believed that this deformity is caused by abnormal fetal position in the uterus, resulting in a postural deformity. Early pathological changes are merely shortening of the abductor muscles. If not treated promptly after birth, it can lead to contracture of the hip abductor and external rotator muscles. However, in some cases, the shortening of the abductor muscles may resolve on its own.
bubble_chart Clinical Manifestations
In a normal infant lying prone with the hips in a neutral position, both iliac crests are at the same level. However, in an infant with abduction hip contracture, when lying prone with the hips in a neutral position, pelvic tilt occurs. The iliac crest on the affected side is significantly lower than that on the unaffected side, the affected lower limb is longer than the unaffected side, the lumbar spinous processes deviate toward the affected side, and there is asymmetry in the gluteal and popliteal creases. However, if the affected limb is abducted to more than 30°, these signs can completely disappear (Figure 1).
Figure 1 Left hip abduction contracture
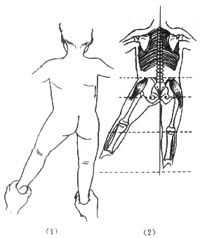
(1)(2) No pelvic or spinous process deviation after left hip abduction
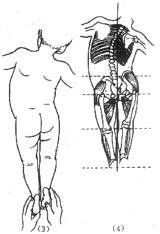
(3)(4) Hip and spinous process deviation after left hip adduction
Radiographic examination may reveal delayed ossification of the acetabular roof on the unaffected side in an anteroposterior pelvic view. This is related to the reduced pressure exerted by the femoral head on the acetabular center due to the adducted position of the unaffected hip. If abduction contracture is not corrected early, it can lead to subluxation of the unaffected hip. Radiographic examination can also rule out other deformities that cause pelvic tilt, such as hemivertebrae in the lumbosacral region or congenital scoliosis.
bubble_chart Treatment MeasuresEarly passive manipulation can achieve complete correction. The best time to treat this condition is within the first two weeks after birth. Persistent passive stretching of the contracted abductor muscles can lead to a cure within four to eight weeks. During the manipulation, place the infant in a prone position, keeping the healthy hip and knee flexed to eliminate lumbar lordosis. The practitioner stabilizes the pelvis and healthy hip with the left hand, holds the affected knee with the right hand, and extends the hip as much as possible, followed by adduction and internal rotation of the hip, maintaining this position for 10 seconds before releasing. Repeat this process about 20 times, performing it four to six times daily. For severe cases of abductor muscle contracture, limb traction and bilateral hip spica cast fixation are required, maintaining the affected hip in adduction, extension, and internal rotation for three to four weeks.
This disease needs to be differentiated from congenital hip dislocation. Patients with congenital hip dislocation often have limited abduction and a positive telescoping test. In contrast, this disease is characterized by increased hip abduction activity and a positive Ober test, making it easy to distinguish from congenital hip dislocation.



