| disease | Chapped Lips |
| alias | Cleft Lip, Harelip |
Chapped lips are a common congenital anomaly in the oral and maxillofacial region, with an incidence of approximately 1 in 1000. In a normal fetus, facial structures begin to form after the fifth week through the gradual fusion of embryonic processes. If this development does not proceed normally, malformations, including chapped lips, can occur.
bubble_chart Etiology
The exact cause and mechanism of disease leading to developmental and fusion disorders are not yet fully understood. According to a large number of experimental studies and epidemiological investigations, it is likely caused by multiple factors rather than a single factor. In summary, it can be divided into two aspects: genetic factors and environmental factors, and is related to nutrition, genetics, infection, endocrine factors, etc.
1. Genetic factors: Patients with chapped lips may find similar deformities in their direct or collateral relatives, thus it is believed that chapped lips deformity is related to genetics to some extent. Epidemiological investigations show that the incidence of chapped lips in offspring is higher in direct relatives with chapped lips deformity than in relatives without cleft deformity. Genetic studies also suggest that chapped lips belong to polygenic genetic diseases.
2. Environmental factors: Mainly refer to the environment of embryonic growth and development, the entire physiological state of the mother constitutes the environmental conditions for embryonic development. Therefore, in the first three months of pregnancy, when the mother's physiological state is invaded or disturbed, it may affect the growth and development of the embryo's maxillofacial region.
(1) Nutritional deficiency: In experimental animal studies, it was found that mice lacking vitamin A, B2 and folic acid and other food components can produce deformities such as chapped lips, but it is not very clear whether humans will also cause congenital deformities due to the lack of these substances. Therefore, nutritional deficiency in early pregnancy may be one of the causes of the disease.(2) Infection and injury: If the mother suffers from some kind of injury in the initial stage of pregnancy [first stage], especially injury that can cause the uterus and its adjacent parts, such as improper incomplete artificial late abortion or unscientific drug early abortion, etc., it can affect the development of the embryo and lead to deformities. The mother suffering from viral infectious diseases such as rubella can also affect the development of the embryo and become a possible cause of chapped lips.
(3) Endocrine influence: Babies born to women in early pregnancy who were treated with hormones due to illness have some congenital deformities. In addition, in the investigation of the family history of children with chapped lips, it was also found that some mothers had various obvious mental trauma factors in early pregnancy, and it is speculated that stress reactions may occur, leading to an increase in the secretion of adrenal cortical hormones in the body, and inducing congenital deformities.
(4) Drug factors: Most drugs can enter the embryo through the placenta after entering the mother. Some drugs may affect the development of the embryo and cause deformities. Currently known anti-tumor drugs (such as cyclophosphamide, methotrexate, etc.), anticonvulsant drugs (phenytoin sodium), antihistamine drugs, and drugs for treating pregnancy vomiting such as meclizine and some sleeping drugs (such as thalidomide) can all cause fetal deformities.
(5) Physical injury: If during the development of the fetus, the pregnant woman is frequently exposed to radiation or microwaves, etc., it may affect the growth and development of the fetus and become a possible cause of cleft lip.(6) Tobacco and alcohol factors: In early pregnancy, heavy smoking and alcohol abuse, the incidence of chapped lips in their children is higher than in women without tobacco and alcohol habits, thus it is also one of the possible factors leading to fetal chapped lips.
bubble_chart Clinical Manifestations
The main manifestation of chapped lips is the splitting of the upper lip. Based on the location and extent of the fissure, it can be classified into grade III.
1. Grade I chapped lips only involve redness and splitting of the lips.
2. Grade II involves a fissure that extends beyond the vermilion border but does not reach the nasal base.
3. Grade III involves a complete fissure from the vermilion border to the nasal base. The first two are also referred to as incomplete chapped lips, while the last one is referred to as complete chapped lips.
(1) Chapped lips can be classified based on the location of the fissure:
1. Unilateral chapped lips are divided into incomplete and complete types.
2. Bilateral chapped lips include incomplete, complete, and mixed types, where one side is complete and the other is incomplete.
(2) Based on the severity of the fissure:
Ⅰ degree chapped lips are limited to the red part of the lips.
Ⅱ degree chapped lips involve partial splitting of the upper lip, not extending to the nasal base. Shallow Ⅱ degree refers to fissures not exceeding half the height of the lip; deep Ⅱ degree refers to fissures exceeding half the height of the lip.
Hidden fissures refer to cases where the skin and mucous membrane are not split, but the muscle layer is missing.
bubble_chart Treatment Measures
(1) Timing of Surgery
It is generally believed that unilateral chapped lips should be operated on around six months, while bilateral chapped lips should be slightly delayed. The basic conditions for the child to be suitable for surgery are: generally good health, no obvious anemia, no upper respiratory tract infection, and no infection in the local and surrounding tissues.
(2) Basic Requirements of Surgery
The basic requirement of chapped lips repair surgery is to restore the normal appearance and function of the lips and nose as much as possible. The normal lips and nose have the following characteristics: both nostrils are equally round and large, the nasal tip and columella are centered, the nasal ala does not collapse, the height of both sides of the upper lip is equal and symmetrical, the vermilion is full, the lip tubercle is slightly protruding, and the vermilion border is arched (Figure 1). The above anatomical features can be used as the basis for the design of chapped lips repair surgery.
|
| 1.3 points indicate the peak points of the vermilion border 2 points indicate the philtrum 1-4,3-5 indicate the philtrum ridges on both sides of the philtrum Figure 1 Normal appearance of the lips and nose |

(3) Surgical Methods for Chapped Lips Repair
The basic steps of chapped lips repair surgery are point design, incision, and suturing. There are many methods of point design. Here, only the lower triangular flap method is introduced. The steps are as follows.
1. Point Design
1) First, find the points on the vermilion border
On the healthy side of the vermilion border, find the peak point D and the lowest point C of the philtrum, then determine point B according to CB=CD. On the affected side of the vermilion border, determine point B′ at the thickest part (Figure 2①). During surgery, points B and B′ are finally sutured together to form the peak point on the affected side (Figure 4).
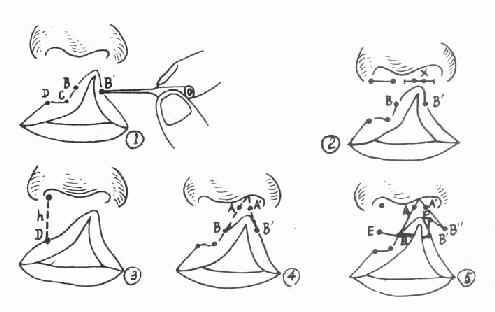
Figure 2 Point design for chapped lips repair surgery
2) Measure two basic data
Measure the width of the normal nostril base and the affected nostril base from the root of the nasal ala to the root of the columella, respectively, to obtain the difference X. Measure h from the midpoint of the healthy nasal base to point D, which is the normal lip height, that is, the upper lip height that should be restored after the repair surgery (Figure 2②③).
3) Determine other points and draw lines
On the affected side of the nasal base, determine points A and A′ on both sides of the cleft. Make AA′ equal to the difference X in the width of the two nostril bases, so that after suturing points AA′, the two nostrils are equal in size. Connect AB. Subtract AB from the normal lip height h to get y, which is the additional lip height needed on the affected side. At point B, make BE approximately equal to y and nearly parallel to the lower lip vermilion border. With A′ as the center and AB as the radius, and B′ as the center and y (the additional lip height) as the radius, draw arcs intersecting at B〞 (preferably B′B〞 is nearly perpendicular to the vermilion border). Then, with B′B〞 as the centers and BE as the radius, draw arcs intersecting at E′. Connect A′B〞, B〞E′, and E′B′ (note not to draw the B′B〞 line, as no incision is made here). After correcting the points, dip a subcutaneous needle in methylene blue and prick into the skin to draw the lines, then fix with iodine (Figure 2④⑤).
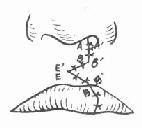
2. Incision and Suturing
The surgery requires meticulousness, gentleness, minimal trauma, accurate incision, and neat suturing.
When making the incision, first use your fingers to firmly pinch the upper lip on the outer side of the incision to reduce bleeding. Then, sequentially cut along the designed lines AB, BE, A′B〞, B〞E′, and E′B〞. After the incision, the healthy side of the upper lip will descend, forming a triangular gap at BE. Insert the triangular tissue flap formed on the affected side, B〞E′B′, into this gap (Figure 3). The wound edge of line AB will align with A′B〞. Proceed to suture layer by layer (Figure 4). Trim the vermilion border, and depending on the situation, use the inlay or Z-plasty method with opposing triangular flaps to enhance the fullness of the vermilion. For nasal deformities, it is generally recommended to postpone radical nasal deformity correction surgery until after the age of 13.
|
|
|
Figure 3 Incision for chapped lips repair | Figure 4 Post-suture for chapped lips repair |

For complete chapped lips with a wider gap and greater tension, an incision should be made in the vestibular groove, followed by undermining to facilitate tissue approximation and suturing.
(4) Postoperative Management
1. A steel wire lip arch with adhesive tape should be applied to the upper lip for 2 weeks to prevent wound dehiscence and reduce scar formation.
2. After the child regains consciousness from basic anesthesia, both elbow joints should be immobilized with splint bandages to prevent scratching the wound and to relieve tension on the lip arch.
3. The lip wound should be gently cleaned with 3% hydrogen peroxide and 4% boric acid alcohol to prevent scab formation, which may affect wound healing.
4. Sutures should be removed 5 days postoperatively.


