| disease | Enterovirus |
| alias | Enterovirus |
Enteroviruses are a group of RNA viruses that can be divided into Coxsackievirus groups A and B, poliovirus, echovirus, and other enteroviruses, with a size of only 20–30 nm. Serological classification can identify 67 types. These viruses can all cause infections through the intestines, so they are collectively referred to as enteroviruses in academic terms. Enteroviruses are found worldwide and often become prevalent in summer and early autumn. They can be transmitted through contact with a patient's oral or nasal secretions, feces, or droplets, and outbreaks frequently occur among children under ten years of age. Although adult cases exist, they are rare. Crowded environments are prone to epidemics. Despite being called enteroviruses, human infections rarely present with intestinal symptoms.
bubble_chart Epidemiology
The primary transmission route of enterovirus is fecal-hand-oral. The virus can be excreted through the patient's sputum, saliva, and feces, and transmitted from one person to another orally. After infection with enterovirus, the virus can be excreted from respiratory secretions and oral secretions 2–3 days before symptoms appear and up to 1–2 weeks after symptoms appear. The virus can persist in feces for several months, potentially infecting others. Enterovirus type 70 can be excreted through tears, while Coxsackievirus A21 is mainly transmitted through respiratory secretions. In areas with poor sanitation, contaminated water and food can also cause outbreaks.
Enteroviruses thrive and spread in warm, humid environments. Taiwan, located in a subtropical region, reports cases of enterovirus infection year-round, making it one of the endemic diseases in the area. Surveillance data from 1998 to 2006 show that young children are at high risk for severe complications and fatalities, with a fatality rate ranging from 10.0% to 25.7% (no deaths were reported in 2006). Enterovirus 71 is the primary serotype causing severe complications, followed by Coxsackievirus. Common symptoms of general enterovirus infections include hand-foot-and-mouth disease or herpangina. Data from a nationwide sentinel physician surveillance system of over 500 sites indicate that enterovirus outbreaks typically begin to rise in late March, peak between late May and mid-June, then gradually decline, with another wave occurring in October. In 2006, the outbreak was delayed by about 3–4 weeks compared to previous years, starting in late April and peaking in late June before gradually subsiding.
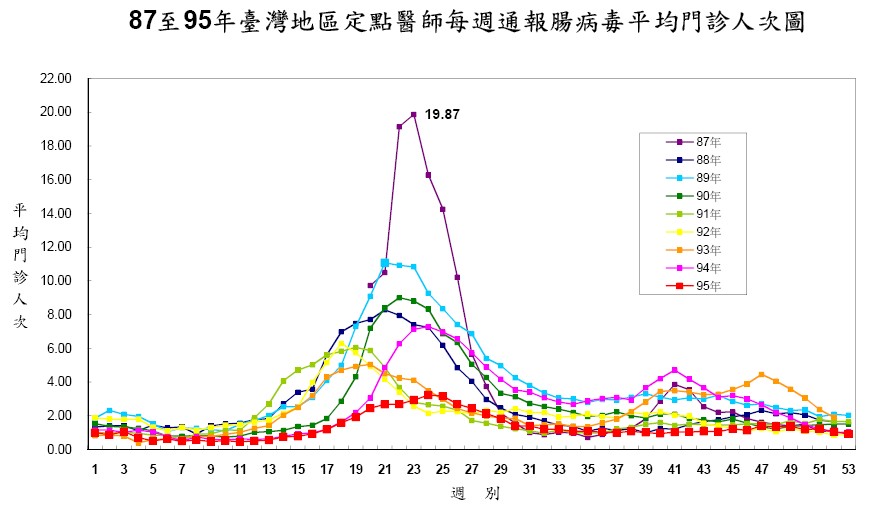
The most severe outbreak occurred in 1998, with the highest average reported cases per sentinel physician reaching 19.87, followed by 2000 with a peak average of 11.08. In subsequent years, the outbreaks became milder. Clinically, herpangina was more common than hand-foot-and-mouth disease in most years, except in 1998 when hand-foot-and-mouth disease predominated.
Age-group analysis shows that over 90% of severe cases (except 88.9% in 1998) occur in children under 5 years old. Fatality rates in fatal cases ranged from 10.0% to 25.7% (no deaths in 2006), with the majority of deaths also occurring in children under 5. The incidence of severe cases is higher in younger age groups, with infants under 1 year old having the highest incidence.
Current Situation in Neighboring Asian Countries
Hong Kong, Singapore, and Japan have established surveillance systems for enterovirus infections to track case numbers and viral serotype trends. Hong Kong and Singapore monitor hand-foot-and-mouth disease, while Japan includes both hand-foot-and-mouth disease and herpangina in its surveillance. Historical surveillance results are as follows:
- Japan: Outbreaks primarily occur in summer, with sentinel physician reports exceeding the alert threshold (1.00 case per physician) between May and June, peaking in mid-July before declining and dropping below the threshold by late August. However, outbreaks have also occurred in autumn and winter. Recent severe hand-foot-and-mouth disease outbreaks were recorded in 1995, 2000, and 2003. The main serotypes causing hand-foot-and-mouth disease are enterovirus 71 and Coxsackievirus A16, while herpangina is mainly caused by Coxsackievirus A10.
- Hong Kong: Outbreaks typically begin in late March to early April, peak in June, and then decline. There are dozens to hundreds of cases annually. Children hospitalized with recurrent╱hand-foot-and-mouth disease showing rapid deterioration, aseptic meningitis╱encephalitis, acute flaccid paralysis, or myocarditis are tested for enterovirus infection. Several to dozens of enterovirus 71 cases are isolated each year.
- Singapore: Since October 1, 2000, hand-foot-and-mouth disease has been classified as a notifiable infectious disease. During the peak of the outbreak in 2000, weekly reported cases reached 1,140. After 2001, the average number of weekly reported cases was about 135, with the majority of patients being children under 4 years old. The predominant virus type was enterovirus 71, followed by coxsackievirus A and echovirus. Enterovirus 71 caused several child fatalities in 2000.
Enteroviruses belong to the Picornaviridae family and are a group of viruses. Before 1997, the known and classified enteroviruses included poliovirus (3 types: 1–3), coxsackievirus (23 types of A: A1–A22, A24, and 6 types of B: B1–B6), echovirus (30 types: 1–33, excluding types 8, 10, and 28), and enterovirus (types 68 and above), totaling over 60 types. In recent years, many additional types have been discovered and reclassified based on genetic sequence analysis into human enterovirus A, B, C, and D. Among these, enterovirus 71 is classified as human enterovirus A.
Among all enteroviruses, aside from poliovirus, enterovirus type 71 (EV71) is the most likely to cause neurological complications. This virus was first isolated during an outbreak in California, USA, in 1969, which resulted in many cases of aseptic meningitis and encephalitis. Since then, outbreaks have been reported in Australia, Japan, Sweden, Bulgaria, Hungary, France, Hong Kong, Malaysia, and other regions. Taiwan also experienced an outbreak over a decade ago, indicating that this virus has a global distribution.
Notably, although reports from around the world have found a particularly high rate of neurological complications following EV71 infection, the severity varies. Some cases involve non-fatal complications such as meningitis, mild encephalitis, or limb paralysis, while others, like the 1998 outbreak in Taiwan, have resulted in fatalities. Similar situations have occurred in Bulgaria, Hungary, Malaysia, and Japan. The potential risk factors require further investigation and research.
In Taiwan, most enterovirus outbreaks are referred to as coxsackievirus because hand, foot, and mouth disease (HFMD) is most commonly caused by coxsackievirus. Different types of enteroviruses can cause various diseases, including HFMD, herpangina, aseptic meningitis, paralytic syndrome, epidemic conjunctivitis, and myocarditis. Some different viruses can also cause the same symptoms, so conditions like HFMD may recur in the same individual multiple times.

Humans are the only source of enterovirus transmission, primarily spread through the gastrointestinal tract (fecal-oral route, water, or food contamination) or respiratory tract (droplets, coughing, or sneezing). Infection can also occur through contact with the fluid from a patient's skin blisters. The virus can be detected in the throat and feces several days before symptoms appear, indicating infectiousness, which is typically strongest within the first week of illness. Patients may continue to shed the virus through the intestines for as long as 8 to 12 weeks.
bubble_chart Clinical Manifestations
The incubation period is 2 to 10 days, with an average of about 3 to 5 days. Most patients are asymptomatic (approximately 50–80%) or only experience fever or symptoms similar to a common cold, recovering naturally within a few days. A small number may develop specific clinical manifestations such as:
- Hand-foot-and-mouth disease (HFMD): Caused by group A coxsackievirus and enterovirus 71, characterized by fever and small blisters on the body, primarily distributed on the oral mucosa and tongue, followed by the soft palate, gums, and lips. On the limbs, they appear on the palms, soles, fingers, and toes. Difficulty eating often occurs due to oral ulcers, and the course of the illness lasts 7 to 10 days.
- Vesicular pharyngitis (herpangina): Caused by group A coxsackievirus. Features include sudden fever, vomiting, and small blisters or ulcers in the pharynx. The illness lasts 4 to 6 days. Most cases are mild without complications, though a few may develop aseptic meningitis.
- Acute myocarditis in infants and pericarditis in adults: Caused by group B coxsackievirus, characterized by sudden dyspnea, pallor, cyanosis, and vomiting. Initially mistaken for pneumonia, it progresses with marked tachycardia, rapidly evolving into heart failure, shock, or even death. Surviving children recover quickly.
- Epidemic pleurodynia: Caused by group B coxsackievirus, featuring sudden paroxysmal chest pain lasting minutes to hours, accompanied by fever, headache, and transient nausea, vomiting, and diarrhea. The illness lasts about a week.
- Acute lymphonodular pharyngitis: Caused by group A coxsackievirus. Symptoms include fever, headache, sore throat, and distinct white lesions on the uvula and posterior pharyngeal wall, persisting for 4 to 14 days.
- Febrile illness with rash: Associated with various types of coxsackievirus and echovirus. The rash is typically maculopapular, though some may develop small blisters.
- Only through laboratory testing can the diagnosis determine which type of enterovirus is responsible, but viral typing does not aid in treatment.
- Most cases with mild symptoms can be managed with symptomatic treatment. For the very few cases with complications, supportive therapy is adopted.
- Patients gradually recover as their immune system overcomes the infection, but the virus can still be excreted in feces for several weeks, potentially infecting others.
- If atypical symptoms such as persistent or recurrent high fever, vomiting, drowsiness, restlessness, confusion, poor activity, cough, or rapid breathing occur, or if there is any doubt, seek medical attention promptly.
- The use of immunoglobulins is still under experimental evaluation, and potential risks must be considered; thus, it should be carefully assessed by a physician.
- After enterovirus infection, immunity can last for a period of time; there may also be short-term cross-immunity against different types of enteroviruses.
- For questions regarding routine vaccinations, especially for infants as young as two months old, consult a physician for careful evaluation before administration.
- First Danger: High-risk group—children under 3 years old. According to 1998 enterovirus outbreak statistics, 78% of fatal cases were under 3 years old.
- Second Danger: Critical period—within 3 days. For severe and fatal cases caused by enterovirus 71, the average time from onset to seeking medical care was 3.4 days. Many cases only reached the emergency room or intensive care unit after the third day, leading to deficient rescue efforts. Thus, the first three days of illness are highly unstable and require close monitoring.
- Third Danger: Three critical symptoms—lethargy, persistent vomiting, and myoclonic spasms. Analysis of fatal and near-fatal cases of brainstem encephalitis caused by enterovirus 71 found these three clinical symptoms to be the most indicative. If present, they must be treated as severe cases.
Enterovirus Disinfection Methods:
- Selection of Disinfection Methods:
- Enteroviruses are resistant to acids and many chemical agents, such as antimicrobials, cleaning disinfectants, and alcohol, which cannot kill enteroviruses.
- Aldehydes and halogen-based disinfectants (such as commercially available chlorine bleach) can deactivate enteroviruses. Residual chlorine in water at 0.3–0.5 ppm can inactivate them, and laundry bleach (containing chlorine) can also kill enteroviruses.
- Enteroviruses can survive at room temperature for several days, for weeks at 4°C, and for months or longer when frozen. However, they quickly lose activity in environments above 50°C. Therefore, heating food or soaking underwear in hot water can reduce the spread of enteroviruses.
- Drying can shorten the survival time of enteroviruses at room temperature.
- Ultraviolet light can reduce viral activity.
- Preparing Disinfectant Solution: Example of Preparing 200 ppm Chlorine Bleach Solution
- Take 1 tablespoon (about 15–20 cc, using a standard soup spoon) of commercially available household bleach (typically 6–7% concentration).
- Add it to 5 liters of tap water (each large plastic bottle is 1250 cc, so 4 bottles equal 5 liters) and mix well.
- Key Points for Environmental Disinfection:
- Large-scale spray disinfection is unnecessary.
- Focus on disinfecting frequently touched surfaces (door handles, desks, dining tables, stair railings), toys, playground equipment, bedding, and books.
- After cleaning, objects can be moved outdoors to be exposed to sunlight.
If accompanied by symptoms such as lethargy, convulsions, persistent vomiting, hospitalization is required due to the risk of complications like aseptic meningitis, pneumonia, myocarditis, pericarditis, and paralysis. Other risk factors include high fever lasting more than three days, blood sugar levels exceeding 150mg/dl, and limb weakness.
- Viral (aseptic) meningitis: Often caused by Coxsackievirus B and echovirus infections.
- Encephalitis: Partially caused by Coxsackievirus A infections.
- Myelitis: Besides poliovirus, enterovirus type 71 infections can also cause it.
- Myocarditis: Approximately 1/3 to 1/2 of myocarditis cases are caused by Coxsackievirus B, mostly occurring in young males and can be fatal.
- Hemorrhagic conjunctivitis: Caused by Enterovirus 70 and Coxsackievirus A24 infections.
- Neonatal infections: Often caused by Echovirus and Coxsackievirus B infections, with a high mortality rate.
Enterovirus-induced herpangina is very similar to vesicular gingivostomatitis (Herpetic Gingivostomatitis), but the ulcers in vesicular gingivostomatitis are located in the front part of the mouth, also causing pain and drooling, but it is not caused by enterovirus infection.
bubble_chart Other Related Items


