| disease | Acute Renal Failure after Burns |
Hypovolemic shock after burns is the main cause of acute renal failure. During shock, the decreased blood pressure or reduced serum sodium in the afferent arteriole stimulates the juxtaglomerular apparatus, leading to the production of large amounts of renin and angiotensin II, which cause renal vasoconstriction, renal ischemia, hypoxia, and a decrease in glomerular filtration rate, resulting in oliguria or even anuria.
bubble_chart Etiology
1. Shock
Hypovolemic shock after burns is the main cause of acute renal failure. During shock, the decreased blood pressure or reduced serum sodium in the afferent arteriole stimulates the juxtaglomerular apparatus, producing a large amount of renin and angiotensin II, which causes renal vasoconstriction, renal ischemia and hypoxia, and a decrease in glomerular filtration rate, leading to oliguria or even anuria.
2. Toxic substances
Severe deep burns and sepsis produce toxic substances, including free hemoglobin, myoglobin, and bacterial toxins, which can directly or indirectly exacerbate renal damage.
3. Antibiotics
Aminoglycoside antibiotics, polymyxin B, and sulfonamides have nephrotoxic effects.
4. Other causes
Severe diarrhea, hot air therapy, and stress-induced diabetes can cause dehydration if not corrected in time. Large doses of vasoconstrictors or diuretics before adequate blood volume replacement during the shock period can predispose to renal insufficiency. Elderly patients and those with pre-existing renal disease are more prone to renal failure.
1. Oliguria
Persistent oliguria after replenishing blood volume and fluids should differentiate between prerenal and postrenal causes.
2. Low specific gravity of urineFixed at 1.010–1.018, with granular casts, epithelial cell fragments, red blood cells, and white blood cells in the urine sediment.
3. Azotemia
Urine urea nitrogen/blood urea nitrogen < 14:1, urine creatinine/blood creatinine < 10:1, blood urea nitrogen/blood creatinine < 10:1.
4. Measurement of free water clearance

The normal value of free water clearance is negative, and the closer it is to zero, the more severe the renal impairment. Free water clearance is more sensitive than blood chemical measurements (BUN, Cr) and aids in early diagnosis.
5. Fractional excretion of sodium (FENa)
In functional renal insufficiency, renal tubules can reabsorb sodium ions extensively, leading to a decrease in FENa. In contrast, with intrinsic tubular damage, the ability to reabsorb sodium ions significantly declines, resulting in an increase in FENa. Thus, FENa can be used to assess the renal tubular capacity for sodium reabsorption, determining the nature and severity of renal insufficiency. The calculation formula is:
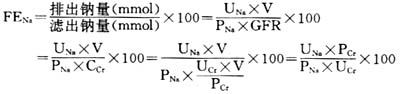
Note: UNa urinary sodium (mmol); P
Na blood sodium (mmol); Cr creatinine clearance; PCr blood creatinine (mg/dl); V urine volume (L); GFR glomerular filtration rate; UCr urinary creatinine (mg/dl); FENa normal value 1–3.
FENa < 1 suggests prerenal or functional renal insufficiency. FENa > 3 indicates acute tubular damage, with renal insufficiency being intrinsic or organic.
bubble_chart Treatment Measures
1. Active and effective anti-shock, anti-infection, and wound management
are key to preventing the occurrence of acute kidney failure. Early excision of necrotic tissue and covering the wound can avoid the release of toxins and infection.
2. Energy supply
After burns, acute kidney failure requires a daily supply of 5000 KCal, which must be achieved through a combination of oral and intravenous nutrition. To reduce fluid intake, concentrated high-calorie intravenous nutrition can be used. Providing a certain amount of essential amino acids to patients with acute kidney failure does not increase urea nitrogen. With sufficient essential amino acids and energy supply, endogenous urea is utilized to reduce the breakdown of endogenous proteins, thereby decreasing hematuria nitrogen and also lowering blood potassium. However, for patients with significantly decreased creatinine clearance, protein supply should be appropriately controlled.
During treatment, it is crucial to prevent excessive fluid infusion. Daily weight measurement and accurate estimation of the patient's fluid intake are necessary.
The fluid requirement for adults with burns combined with ARF = 500ml + 24-hour urine output + gastrointestinal loss + surface evaporation loss + additional loss.
Additional losses include 1000ml from tracheostomy and 2000-3000ml from the use of hot air blowers.
4. Dialysis treatment
Commonly used methods include peritoneal dialysis and hemodialysis. Peritoneal dialysis is simple and easier to control fluid overload with hypertonic dialysis solution, without dietary restrictions. However, peritoneal dialysis takes a long time, is inconvenient for turning and wound management, and results in more loss of albumin and amino acids; it is also prone to complications of abdominal and thoracic infections.
Hemodialysis requires arteriovenous fistula surgery; blood must be heparinized when passing through the dialyzer, making the operation relatively more complex. However, hemodialysis has shorter dialysis times, which is beneficial for wound management, and there is no risk of abdominal and thoracic infections. Moreover, hemodialysis is effective and fast.
Indications for dialysis: ① Serum potassium higher than 6.5mEq/L; ② Water intoxication, congestive heart failure, pulmonary edema, cerebral edema, soft tissue edema; ③ Hematuria nitrogen greater than 100mg/dl or a daily increase of 30mg/dl; ④ Progressive acidosis, CO 2 -CP < 15mmol/L or blood pH < 7.15.



