| disease | Congenital Radial Aplasia |
| alias | Club Hand |
Congenital radial deficiency is also known as club hand. It was first reported by Petit in 1733, with the severity of the deformity ranging from simple radial dysplasia to complete absence of the radius. The incidence is approximately 1 in 100,000. About half of the patients have bilateral involvement. In unilateral cases, the right side is affected twice as often as the left, with a male-to-female ratio of 1.5:1.
bubble_chart Etiology
The true cause of congenital radial deficiency remains unclear. According to Gegenbauer's theory, the upper limb consists of a main axis and four accessory rays. The first accessory ray is composed of the radius, scaphoid, trapezium, first metacarpal, and the two phalanges of the thumb. When the development of the first accessory ray is inhibited, congenital radial deficiency occurs, often accompanied by the absence of the thumb.
bubble_chart Pathological Changes
1. This deformity can be divided into three types. Type A is radial dysplasia. The distal radial growth plate is absent, with delayed epiphyseal ossification, a shortened distal radius, and the radial styloid process at the same level as the ulnar styloid process. The proximal radial epiphysis maintains a normal relationship with the elbow joint. The radial shortening is mild, with dysplasia of the scaphoid and trapezium, and the thumb may be small or absent. The wrist exhibits radial deviation but remains relatively stable. Type B is partial absence of the radius (Figure 1A), where the middle and distal portions of the radius fail to develop, while the proximal radius remains normal, providing some stability to the elbow joint. The radius is hypoplastic and fused with the ulna, forming a type of radioulnar synostosis. Occasionally, the radius may fuse with the capitulum of the humerus. The ulna is shortened, thickened, and curved, convex toward the radius. The wrist joint is unstable, with radial deviation of the hand. Type C is complete absence of the radius (Figure 1B). This is the most common type, accounting for approximately 50% of such deformities. Due to the lack of radial support at the wrist, the radial soft tissues of the forearm are severely contracted, resulting in radial deviation of the hand and forearm at 90° or more. When the elbow is flexed, the hand may even become parallel to the upper arm. The radial ray bones are completely absent, including the scaphoid, trapezium, first metacarpal, and thumb bones. If the thumb is present, it is often hypoplastic or floating. The humerus is shortened, with hypoplasia or absence of the capitulum, and delayed ossification of the distal humeral epiphysis.
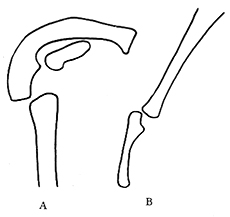
Figure 1 A. Type B absence of the radial head B. Type C absence of the radial head
2. The ulnocarpal connection is fibrous, lacking articular cartilage coverage, and the wrist joint is dislocated radially and volarly, with significant contracture of the radial soft tissues of the forearm. If left untreated, the deformity worsens with skeletal growth. The metacarpophalangeal joints exhibit hyperextension and limited flexion, while the proximal interphalangeal joints develop fixed flexion deformities. Radiographs of the proximal interphalangeal and metacarpophalangeal joints appear normal. Joint stiffness may be related to abnormalities of the extensor tendons. The severity of digital contractures decreases progressively from the radial to the ulnar side.
In one-fourth of cases, the elbow joint is stiff in extension. If elbow extension contracture cannot be corrected, it is considered a contraindication for wrist centralization surgery.
Muscles are similarly affected. The radial extensors may be absent, hypoplastic, fibrotic, or fused. The pronator quadratus, extensor carpi radialis longus and brevis, brachioradialis, and supinator muscles are often absent. The flexor pollicis longus, extensor pollicis longus and brevis, abductor pollicis brevis, and thenar muscles are also frequently absent. However, the interossei, lumbricals, and hypothenar muscles are usually unaffected.
The wrist and finger extensors are present but often fused. The flexor digitorum superficialis exhibits significant variability, ranging from hypoplasia to fibrosis or fusion with the flexor digitorum profundus.
The long head of the biceps is absent, while the short head remains but has an abnormal insertion, often attaching to the joint capsule, remnants of the radius, or the medial epicondyle of the humerus. The pectoralis major and minor and deltoid muscles are present but may have abnormal insertions or fuse with the deltoid or brachialis.
3. Nerve involvement: The axillary and ulnar nerves are normal, while the musculocutaneous nerve is often absent. The radial nerve typically terminates at the elbow, with the radial sensation of the hand supplied by the median nerve. The median nerve is thicker than normal and lies beneath the deep fascia on the radial side of the forearm. Care must be taken during surgery to avoid injury.

4. Vascular involvement: The ulnar artery is present and often serves as the primary blood supply to the forearm and hand. The interosseous artery is well-developed. The radial artery and palmar arch are abnormal, with the degree of vascular involvement correlating with the severity of radial dysplasia. The radial side of the forearm is supplied by the anterior interosseous artery, which arises from the ulnar artery and accompanies the median nerve. The radial artery is regressed or absent.
bubble_chart Clinical Manifestations
The forearm is short and curved radially, with a spherical protrusion distally at the site of the ulnar styloid process. The radial styloid process is not palpable, and the hand exhibits radial deviation. The degree of functional loss varies depending on whether the condition is unilateral or bilateral. In unilateral cases, although the affected limb is clumsy, compensatory use of the unaffected contralateral upper limb generally allows the individual to perform daily activities. Bilateral involvement results in greater functional impairment, with difficulties in daily tasks such as dressing, eating, and bathing. Limited elbow flexion exacerbates functional loss. The radial two fingers exhibit flexion contractures and reduced mobility, while the ulnar two fingers remain normal with good function. The thumb is absent, the index finger deviates ulnarly, and the little finger deviates radially.
The diagnosis can be made based on clinical manifestations and X-ray imaging.
bubble_chart Treatment Measures
1. The treatment plan is determined based on the degree of radial longitudinal deficiency.
For Type A patients, Gypsum orthosis is used to correct the soft tissue contracture on the radial side of the forearm. Passive stretching exercises are performed to maintain the functional position of the wrist. At 8–10 years of age, if radial shortening progresses and affects wrist function, a radial "Z" osteotomy for lengthening and complete soft tissue release are performed. Postoperatively, the upper limb is immobilized with Gypsum, with the elbow flexed at 60°–70°, the forearm in supination, and the wrist in the functional position. Gypsum immobilization lasts for 8–10 weeks.
For Type B or C patients, due to wrist instability, severe radial deviation, and palmar flexion of the hand, treatment should begin immediately after birth to prevent soft tissue contracture. After Gypsum correction, if the hand reaches a neutral position, nighttime splinting is initiated, along with passive flexion exercises of the elbow, palmar flexion of the metacarpophalangeal joints, and hyperextension of the proximal interphalangeal joints.
If radial deviation of the hand and wrist instability worsen, affecting hand function, centralization surgery of the wrist is performed. This includes tightening the ulnar and dorsal joint capsules of the wrist, tendon transfer of the hand, radial soft tissue release, and, if necessary, ulnar wedge osteotomy to correct the bending deformity. The optimal timing for surgery is during infancy.
2. Contraindications for wrist centralization surgery include: ① Concurrent severe deformities, such as Fanconi’s pancytopenia, which pose significant surgical risks. ② Elbow extension contracture, where even if hand function is reconstructed, the inability to flex the elbow prevents functional use of the hand. ③ Older patients, such as adolescents or adults, who have fully adapted to the deformed hand, exhibit severe ulnar bending, and progressive shortening and pathology of blood vessels and nerves. Even if surgical correction is performed, patients may struggle to adapt and are at high risk of severe complications.
Severe combined malformations, such as Fanconi's pancytopenia (Fanconi's refractory anemia).


