| disease | Wrist Joint Tuberculosis |
Subcutaneous nodules of the wrist joint rank third among the upper limb joints, accounting for 0.43/100 of all patients with bone and joint subcutaneous nodules. They are more common in adults. Like other limb joints, patients often have subcutaneous nodule lesions in other areas simultaneously.
bubble_chart Pathological Changes
The wrist joint has a complex structure, connecting the forearm and the wrist joint. Proximally, it consists of the distal ends of the radius and ulna along with the triangular fibrocartilage. In the middle are the eight carpal bones, and distally, the bases of the metacarpal bones. The eight carpal bones are divided into two rows: the proximal row includes the scaphoid, lunate, triquetral, and pisiform bones, while the distal row comprises the trapezium, trapezoid, capitate, and hamate bones. Except for the pisiform bone, the other carpal bones have more than one articular surface. The capitate bone has articular surfaces with all seven adjacent bones, earning it the title of the "key" to the wrist joint. Once a subcutaneous nodule forms on the capitate bone, it can easily spread to adjacent joints, leading to a full-joint subcutaneous nodule.
The ossification centers of the carpal bones appear relatively late, with roughly one appearing each year within the first five years after birth. As a result, subcutaneous nodules in the wrist joint are rare in children under 10 years old. Among 103 cases in Tianjin, only 7 were children under 10.
The movements of the carpal bones include dorsiflexion, palmar flexion, radial deviation, ulnar deviation, and rotational motion.
bubble_chart Clinical Manifestations
The wrist joint is composed of four joint cavities: the ulnoradial, radiocarpal, intercarpal, and carpometacarpal. In the early stages, pain and swelling of the subcutaneous node begin at a specific point or within one joint cavity; whereas wind-warmth primarily invades the synovial membrane, with generalized swelling being its characteristic feature. Among the carpal bones, the ossification center of the capitate bone appears first. When the subcutaneous node is initially infected via hematogenous spread, it is the first to be affected, making the capitate bone the most frequently involved in subcutaneous node infections, followed by the hamate and trapezium bones. The lesion tends to spread to the small intercarpal joints, affecting the metacarpal bones and the extensor tendon sheaths of the wrist, leading to extensive destruction and the formation of abscesses and sinuses on the dorsum of the hand. The wrist joint has little synovial membrane, so isolated synovial membrane subcutaneous node infections are rare.
In the early stages, swelling occurs on the dorsal side of the wrist joint, followed by pain and impaired mobility. Severe destruction of the wrist joint can lead to wrist drop and ulnar deviation deformities.bubble_chart Auxiliary Examination
In the early stage of X-ray imaging, simple synovial subcutaneous nodules may reveal osteoporosis and soft tissue swelling. The distal ends of the ulna and radius may exhibit subcutaneous nodules with central sequestrum or marginal osteolytic destruction. In the advanced stage, extensive destruction of multiple carpal bones, the distal ends of the ulna and radius, and the articular surfaces of the metacarpal bones can be observed. Deformities of the wrist joint may also appear.
The diagnosis can be made based on medical history, clinical manifestations, and X-ray imaging.
bubble_chart Treatment Measures
Fix the wrist joint in the functional position with a Gypsum splint. For cases where drug therapy is ineffective, a dorsal longitudinal S-shaped incision can be used to perform synovectomy and lesion debridement (Figure 1). For subcutaneous nodules at the distal ends of the ulna and radius, corresponding incisions should be made based on the lesion's location. In cases of severe carpal bone destruction, resection of the distal or proximal row of carpal bones, or even total wrist arthrectomy, may be performed. Postoperatively, the wrist should be immobilized in the functional position with a Gypsum splint for 3–4 weeks.
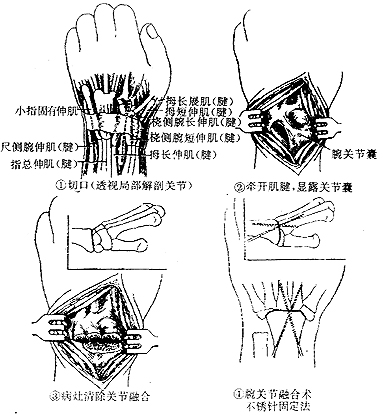
Figure 1 Wrist joint lesion debridement.
There are also subcutaneous nodular lesions in other areas.
Early-stage lesions, particularly simple synovial subcutaneous nodules, are difficult to differentiate from solitary rheumatic wrist arthritis.


