| disease | Shoulder Joint Tuberculosis |
The shoulder joint subcutaneous node has the lowest incidence among the three major joints of the upper limb, with a total of 21 cases accounting for 0.51% of patients treated during the same period. Most cases occur in young adults, and patients often also have active pulmonary subcutaneous nodes.
bubble_chart Pathological Changes
The shoulder joint is a ball-and-socket joint, which is the joint with the most movement directions and the largest range of motion in the human body. It is formed by the bones and the glenoid cavity of the scapula. The posterior part of the scapula is the acromion, and the anterior part is the coracoid process. These two protrusions are connected by the weak coracoacromial ligament to form the shoulder arch, which is covered by the deltoid muscle to limit the rules of arm elevation and abduction.
The articular surface of the scapula itself is surrounded by a fibrocartilaginous ring, making the glenoid cavity deeper and broader.
Range of motion of the shoulder joint: Normal abduction and forward flexion can reach 180°, adduction 50°, backward extension 40°, external rotation 60°–80°, and internal rotation 100°–110°.
The anterior, posterior, and lateral aspects of the shoulder joint are all covered by the deltoid muscle, with the axillary fossa located below, filled with fat and neurovascular structures. When exposing the shoulder joint, part of the deltoid muscle must be incised to access the joint, but care must be taken not to injure the axillary nerve, which runs from posterior to anterior deep to this muscle, otherwise the deltoid muscle will atrophy.
bubble_chart Clinical Manifestations
The shoulder joint is surrounded by abundant muscles with good local blood supply, making abscesses prone to absorption. Therefore, shoulder joint subcutaneous node was once referred to as dry bone ulcer, but it is relatively rare.In the early stage, there is dull pain in the shoulder, which worsens with exertion, and the upper limb often assumes an adducted position. When a simple bone subcutaneous node progresses to a full-joint subcutaneous node, the inflammatory exudate increases, raising the intra-articular pressure and intensifying the pain. Subsequently, pus may rupture the joint capsule, reducing intra-articular pressure and alleviating local pain. However, if secondary suppurative infection occurs in the sinus, local pain worsens again. By the advanced stage, fibrous ankylosis of the joint eliminates the pain.
In cases of simple bone subcutaneous node, shoulder joint movement is only grade I restricted. In full-joint subcutaneous node, functional impairment is significant: the affected arm cannot be raised, and external rotation, abduction, flexion, and extension are all limited. Atrophy of the deltoid, supraspinatus, and infraspinatus muscles leads to a "square shoulder" deformity. Due to the weight of the upper limb, the humeral head often exhibits downward subluxation.
Full-joint subcutaneous node is more common. Abscesses may extend along the bicipital groove to the inner side of the upper arm or appear in front of, behind, or within the armpit, often rupturing to form a sinus.
bubble_chart Auxiliary Examination
Plain X-ray of the shoulder joint shows only localized osteoporosis and soft tissue swelling in the synovial membrane and subcutaneous nodules, sometimes with widening of the joint space. Lesions in the acromion, glenoid, or humeral head often present as central destruction or sequestrum formation. Lesions in the greater tuberosity of the humerus may appear as central destruction, localized marginal blurring, or bone destruction. In advanced stages, the entire joint is affected, with severe destruction of the joint, narrowing of the joint space, deformation of the humeral head, and sometimes subluxation.
bubble_chart DiagnosisThe diagnosis can be easily made based on medical history, signs, and radiographic findings.
bubble_chart Treatment Measures
Systemic anti-subcutaneous node drug therapy. For simple synovial membrane subcutaneous nodes, anti-subcutaneous node drugs can be injected through the needle inserted anterior to the joint, outside and below the coracoid process. If ineffective, synovial membrane resection should be performed. Enter the joint via the anterior approach, remove only the synovial membrane tissue during surgery, preserve the fibrous layer of the joint capsule, rinse thoroughly, and suture layer by layer, ensuring the fibrous layer is sutured. Postoperatively, the affected limb should be suspended with a triangular bandage for 3 weeks before initiating functional exercises. For simple bone subcutaneous nodes, surgical approaches vary depending on the lesion site, with the anteromedial approach being commonly used (Figure 1). In advanced-stage whole-joint subcutaneous nodes, perform lesion debridement and fuse the shoulder joint in a functional position of 40° abduction, 30° flexion, and 25° external rotation. Postoperatively, fix with a shoulder spica cast or abduction brace for 4–6 months.
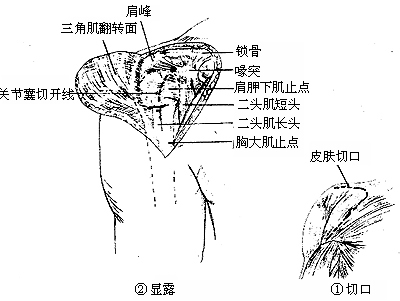
Figure 1 Anteromedial approach for shoulder joint lesion debridement
① Incision ② Retracting the deltoid to expose the shoulder joint
Often associated with active pulmonary subcutaneous nodules.


