| disease | Myocardial Infarction Complicated by Left Ventricular Aneurysm |
After myocardial infarction in the left ventricle, the entire thickness of the ventricular wall myocardium undergoes necrosis. In approximately 10-38% of cases, the necrotic myocardium is gradually replaced by fibrous scar tissue, forming a ventricular aneurysm. The thinned ventricular wall in the affected area bulges outward, losing its ability to contract or exhibiting paradoxical movement during systole. As early as 1881, the progression of coronary artery obstruction, myocardial infarction, myocardial fibrosis, and left ventricular aneurysm was well understood. The clinical diagnosis of left ventricular aneurysm advanced rapidly starting in the 1960s. In 1955, Likoff and Bailey pioneered closed resection of ventricular aneurysms. In 1958, Cooley successfully performed the first ventricular aneurysm resection under cardiopulmonary bypass.
bubble_chart Pathological Changes
Approximately 85% of left ventricular aneurysms are located in the anterolateral region near the apex, while a minority of cases may occur on the diaphragmatic surface of the heart. The affected ventricular wall becomes thin, appearing as a white fibrous scar with clear boundaries, and the local epicardium adheres tightly to the pericardium. About half of the cases exhibit mural thrombi on the endocardial surface, sometimes showing calcification. Coronary artery obstructive lesions are mostly confined to the left anterior descending branch but may also involve multiple vessels. The left ventricular cavity enlarges, and the unaffected myocardium undergoes hypertrophy.
Left ventricular aneurysms cause the loss of contractile ability in the affected area and may produce paradoxical pulsation. During ventricular systole, the aneurysm bulges outward, and during diastole, it retracts, leading to a reduction in left ventricular stroke volume. The normal myocardium increases its contractile force and tension, resulting in higher oxygen demand. When the aneurysm volume exceeds 15% of the left ventricular end-diastolic volume, the end-diastolic pressure of the left ventricle rises. Impaired left ventricular ejection function leads to progressive left heart failure. If a thrombus within the aneurysm dislodges, systemic embolism may occur.
bubble_chart Clinical ManifestationsLeft ventricular wall tumor diseases are mostly associated with a history of colicky pain and myocardial infarction. Common clinical manifestations include dyspnea, left heart failure, colicky pain, arrhythmia, and systemic stirred pulse embolism. The severity of clinical symptoms is closely related to the size of the ventricular aneurysm and the quantity and functional status of the normal myocardial tissue in the left ventricle.
Physical examination: A diffuse systolic lift or double pulsation may be palpated in the apical region. Auscultation may reveal the presence of the third or fourth heart sounds.
bubble_chart Auxiliary Examination
Chest X-ray examination reveals localized bulging at the apex of the left heart border, weakened or paradoxical pulsation, pulmonary congestion, and enlargement of the left atrium and left ventricle.
Electrocardiogram (ECG) often shows old anterior wall myocardial infarction, bundle branch block, and ST-segment elevation.
Long-axis left ventricular echocardiography demonstrates localized bulging of the affected myocardial area, with paradoxical movement of the aneurysmal wall compared to the normal left ventricle during cardiac systole and diastole.
Selective left ventriculography can reveal the location and size of the ventricular aneurysm, the presence of thrombus within the aneurysm, and allows measurement and calculation of left ventricular end-diastolic pressure, ejection fraction, and end-diastolic volume.
Selective coronary angiography can display the location and severity of lesions in the coronary artery branches, providing crucial information for formulating a surgical treatment plan.

Surgical Indications: Patients with a large left ventricular aneurysm presenting clinically with congestive heart failure, cardiac colicky pain, ventricular tachycardia, and systemic embolism should be considered for surgical treatment. For cases with cardiac colicky pain, coronary artery bypass grafting should be performed concurrently based on the condition of the coronary artery branch lesions during the aneurysm resection. Cases with severe heart failure symptoms that are difficult to control with medical therapy, a large aneurysm occupying more than 50% of the left ventricular free wall, multiple coronary artery lesions, and generalized weakening of left ventricular myocardial contractility in non-aneurysmal areas have a high surgical mortality rate and should be carefully evaluated. Small aneurysms without significant clinical symptoms can generally be closely monitored for progression and do not require urgent surgical intervention.
**Surgical Technique for Aneurysm Resection:** The procedure is performed under extracorporeal circulation combined with hypothermic cardioplegia. A midline sternotomy is performed, and the pericardium is incised. Cannulas are inserted into the superior and inferior vena cava via the right atrium and right atrial appendage, and an arterial cannula is placed in the ascending aorta. After cross-clamping the ascending aorta, localized deep hypothermia is induced, and cold cardioplegic solution is infused into the ascending aorta. Before cardiac arrest, manipulation of the aneurysm should be avoided to prevent thrombus dislodgement and embolism. If adhesions between the aneurysm and pericardium are loose, they can be dissected. However, if the adhesions are dense and difficult to separate, the aneurysm can be incised along with the pericardial membrane. The thrombus and mural clots within the aneurysm cavity are removed, and gauze may be placed in the left ventricular cavity to prevent clot migration into the aorta or left atrium. The mitral valve, papillary muscles, and the interface between the fibrotic scar tissue of the aneurysm and the normal left ventricular myocardium are identified. The aneurysm is excised approximately 0.5 cm from this interface. The remaining fibrous rim of the aneurysm can be used to reinforce the ventricular closure, and normal myocardium should be preserved as much as possible. The ventricular cavity is irrigated with saline, and after removing debris, the left ventricular incision is closed in two layers using heavy silk or 1-0 polyester sutures. The first layer consists of interrupted or continuous mattress sutures with polyester pledgets, and the second layer is either interrupted or continuous. If the myocardial tissue is fragile, long polyester strips can be placed on both sides of the incision to reinforce the sutures. Care must be taken to avoid injuring the papillary muscles and to prevent ligation of the left anterior descending coronary artery during closure. For cases where the aneurysm involves part of the interventricular septum, the fibrotic and weakened septum should be reinforced or patched to prevent paradoxical motion postoperatively. The scarred septal region can be sutured to the left ventricular wall adjacent to the right edge of the incision before closing the aneurysm. If the fibrotic area of the septum is large, interrupted sutures can be used to plicate the weakened region, or a patch can be sewn to reinforce the septum before closing the aneurysm, with sutures passing through the anterior edge of the patch (Figure 1).


(1) Incising the aneurysm
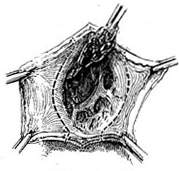
(2) Removing thrombus and excising the aneurysm
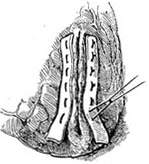
(3) Suturing the incision with pledgets

(4) Reinforcing the sutures
**Figure 1** Resection of ventricular aneurysm
Before completely suturing the ventricular aneurysm incision, fill the left ventricular cavity with saline to expel residual air. Prior to releasing the aortic cross-clamp, insert venting needles into the left ventricle and ascending aorta for decompression and air removal. After rewarming to above 35°C and restoring heartbeat, discontinue cardiopulmonary bypass. Place pacing electrodes on the right ventricle to facilitate postoperative management of arrhythmias. For cases requiring concomitant coronary artery bypass grafting, harvest the great saphenous vein during thoracotomy for later use. After resecting the ventricular aneurysm, first perform the distal anastomosis of the great saphenous vein to the coronary artery branch. Following removal of the aortic cross-clamp, partially clamp the ascending aortic wall to perform the proximal anastomosis of the great saphenous vein to the ascending aorta.
Surgical treatment outcomes: In recent years, the surgical mortality rate has dropped below 10%. The main causes of early postoperative death are acute heart failure, low cardiac output syndrome, severe arrhythmia, and cerebrovascular embolism. Postoperative symptoms have significantly improved, with a 7-year survival rate of 60-80%. The postoperative survival rate for single-vessel disease is higher than that for multi-vessel disease.
The prognosis of left ventricular aneurysm is closely related to the extent of myocardial involvement and the size of the aneurysm. Patients with small aneurysms, limited myocardial involvement, and no clinical symptoms or only grade I dyspnea may survive for more than 10 years after acute myocardial infarction. However, in cases with extensive lesions that severely impair left ventricular systolic ejection function, significantly reduced ejection fraction, and clinical manifestations of congestive heart failure, the 5-year survival rate drops to approximately 10-20%.


