| disease | Masseteric Space Infection |
Masseteric space infection refers to the suppurative infection of the masseteric space, with the main clinical manifestations being acute inflammatory redness, throbbing pain, and tenderness centered around the masseter muscle.
bubble_chart Etiology
The masseteric space is located between the masseter muscle and the lateral bony wall of the mandibular ramus. Due to the broad and tight attachment of the masseter muscle to the mandibular ramus and its angle, the potential masseteric space exists in the lateral portion of the upper segment of the mandibular ramus. It connects with the buccal, infratemporal, pterygomandibular, and temporal spaces via fatty connective tissue (Figure 2). The masseteric space is one of the most common sites of maxillofacial space infections.
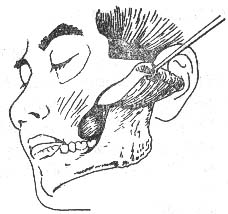
Figure 2 Anatomical location of the masseteric space
bubble_chart Clinical Manifestations
The infratemporal space is deep and concealed, so infections in this area often show no obvious external signs. Careful examination may reveal slight swelling above and below the zygomatic arch or behind the mandibular ramus, with deep tenderness and varying degrees of restricted mouth opening. However, infections in the infratemporal space frequently involve adjacent spaces, leading to swelling in the temporal region, masseteric-parotid area, cheek, or the maxillary tuberosity region inside the mouth, along with corresponding symptoms of the combined space infections.
1. Medical History: History of acute suppurative pericoronitis of the mandibular wisdom tooth.
2. Clinical Manifestations: Acute inflammatory redness, throbbing pain, and tenderness centered around the masseter muscle. The area of redness extends above the zygomatic arch, below to the submandibular region, anteriorly to the cheek, and posteriorly to the retromandibular area. Deep pressure reveals pitting edema, with difficulty palpating fluctuation. Severe trismus is present. A thick needle inserted into the center of the redness can aspirate a small amount of thick pus when the needle tip reaches the bone surface and is slowly withdrawn. The patient has high fever, elevated total white blood cell count, and an increased proportion of neutrophils.
bubble_chart Treatment MeasuresFor masseteric space cellulitis, in addition to systemic antibiotics, local physical therapy or topical application of Chinese medicinals can be used. Once an abscess forms, timely drainage should be performed. The approach for incision and drainage of a masseteric space abscess can be made intraorally by incising slightly lateral to the pterygomandibular fold and dissecting into the abscess cavity for drainage. However, because the drainage opening is often located in the anterior-superior part of the abscess cavity, postural drainage is inadequate, inflammation is difficult to control, and the risk of marginal osteomyelitis increases accordingly. Therefore, the extraoral approach is commonly used clinically for incision and drainage. The extraoral incision is made from the posterior border of the mandibular ramus, curving around the mandibular angle, and incising 2 cm below the lower border of the mandible. The incision is approximately 3–5 cm long. The subcutaneous tissue, platysma muscle, and part of the masseter muscle attachment in the mandibular angle area are incised layer by layer. A periosteal elevator is used to lift the masseter muscle from the bone surface to enter the abscess cavity, drain the pus, and irrigate the cavity before packing it with saline gauze for drainage (Figure 1). The next day, during dressing change, the gauze is removed and replaced with a rubber tube or rubber strip for drainage. If marginal osteomyelitis develops, early curettage of the sequestrum should be performed once pus discharge decreases. During the procedure, in addition to focusing on removing sequestra from the bone surface, small fragments of sequestra and necrotic tissue attached to the periosteal surface beneath the masseter muscle should not be overlooked to promote early wound healing.
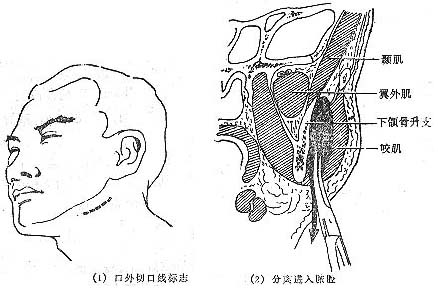
Figure 1 Extraoral incision and drainage of a masseteric space abscess.



