| disease | Urachal Cyst and Urachal Fistula |
Urachal cysts and urachal fistulas are both relatively rare. However, it is not uncommon to find a tent-shaped depression at the midline apex of the bladder or an incompletely obliterated urachal segment in the lower abdomen during clinical surgery. Of course, such conditions do not typically present as clinical issues.
bubble_chart Pathogen
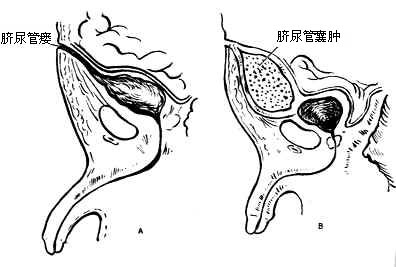
The etiology of this disease occurs when the embryo is 10–24 mm in size, and the bladder is still enlarged to the umbilicus. Subsequently, the bladder descends along the anterior abdominal wall. During this descent, a fine duct remains connected to the urachus. This duct gradually narrows, occludes, and becomes a fibrous cord extending from the umbilicus to the anterior wall of the bladder. If it does not fully occlude and retains a lumen, it becomes a urachal fistula. If both ends are occluded while the middle portion remains incompletely closed, there is a possibility of cyst formation (Figure 1).
bubble_chart Clinical Manifestations
Urachal fistula manifests as a persistently moist umbilicus with thin secretions. Urachal cyst presents as a cystic mass in the midline of the lower abdomen that does not change with body position.
Urachal fistula manifests as a persistently moist umbilicus with thin secretions, suggesting the possibility of this condition. If there is a significant amount of clear, watery discharge, it is more likely to be a urachal fistula, which can be confirmed by injecting indigo carmine into the bladder. If the discharge is scant and mucoid, an omphalomesenteric fistula is far more probable than this condition, requiring further differentiation. Urachal cyst presents as a cystic mass in the midline of the lower abdomen, which does not shift with changes in body position, is superficial, and closely related to the abdominal wall. Ultrasonography can confirm these characteristics.
bubble_chart Treatment MeasuresIf there is no infection, surgical resection is recommended. If infection is already present, active treatment of the infection should be carried out, followed by surgical resection after the infection is controlled.



