| disease | Nasal Bone Fracture |
Nasal bone fractures are mostly caused by trauma, clinically presenting with nasal laceration and epistaxis, and can be either closed or open. They are often accompanied by fractures of other facial bones or the skull base.
bubble_chart Clinical Manifestations
1. Epistaxis
At the time of nasal bone fracture, there is almost always a tear in the nasal mucosa and epistaxis.
2. Local deformity
When the force comes from one side, the nasal bone on the same side collapses inward, while the opposite side protrudes, resulting in a deviated nose deformity. A frontal impact often causes bilateral nasal bone fractures, leading to a collapsed nasal bridge and saddle-shaped deformity. Within 2–4 hours after the injury, swelling and bruising of the nasal soft tissues and eyelids may temporarily mask the deformity. In cases accompanied by nasal septum dislocation or fracture, the nasal septum or exposed cartilage in the nasal cavity may be visible (Figure 1).
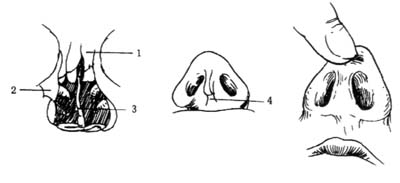
Figure 1 Nasal bone fracture and dislocation (1. Nasal bone fracture; 2. Fracture of the frontal process of the maxilla; 3. Nasal septum fracture; 4. Fracture of the anterior nasal spine; 5. Nasal septum dislocation)
3. Tenderness and crepitus
Pain is not severe after a nasal bone fracture, but there is obvious tenderness at the fracture site, and crepitus can often be felt. When palpating the lower edges of both nasal bones simultaneously with two fingers, the fractured side loses its normal firm resistance. If the patient blows their nose after the injury, air may escape through the mucosal tear and spread to the nasal dorsum and ipsilateral eyelid, potentially causing subcutaneous crepitus.
Open nasal bone fractures usually result from more severe trauma, often presenting as comminuted fractures and frequently accompanied by other craniofacial fractures. Foreign bodies may remain in the wound. If accompanied by a cribriform plate fracture, cerebrospinal fluid rhinorrhea may occur, which warrants attention.When the diagnosis of a nasal bone fracture is unclear, a lateral X-ray can help determine the location of the fracture line and the displacement of bone fragments.
bubble_chart Treatment Measures
For a simple nasal bone fracture without displacement, only hemostasis is required without further treatment. If bleeding has stopped, a 10% mild silver protein solution can be administered as nasal drops. Early cold compresses should be applied to the external nasal swelling, switching to warm compresses after 24 hours. Nose blowing is prohibited to prevent subcutaneous emphysema. If displaced fragments cause deformity, reduction should be attempted before nasal swelling occurs. If severe swelling is already present, reduction may be appropriately delayed but should not exceed two weeks post-injury.
1. Closed Reduction of Nasal Bone Fracture
Place cotton strips soaked in anesthetic containing adrenaline on the nasal mucosa surface for 5–10 minutes, then remove them before proceeding with the procedure. Insert a nasal septum elevator or bayonet forceps wrapped with Vaseline gauze or cotton (Figure 2) into the nose, positioning it behind the nasal bone. Apply upward and forward force to lift the displaced fragment, during which an audible reduction sound may be heard (Figure 3). For bilateral nasal bone fractures or fractures/dislocations of the nasal septum, nasal bone reduction forceps are preferred. Insert the blades of the forceps behind both nasal bones, ensuring they do not extend beyond the line connecting the inner canthi. Simultaneously lift the depressed nasal bones on both sides and realign the nasal septum while the other hand molds the nasal bridge to assist reduction (Figure 4). Alternatively, a finger may be gently inserted through the nostril to manually reposition the fractured nasal septum. After reduction, pack the nasal cavity with Vaseline gauze for 24–48 hours. Avoid pressure on the fracture site for two weeks.

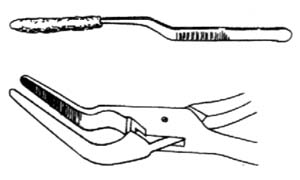
Figure 2: Nasal bone reduction forceps and alternative nasal forceps
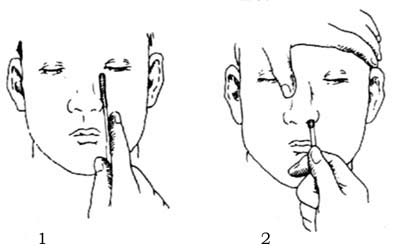
Figure 3: Elevator reduction method (1. First assess the depth of the fracture; 2. Position the elevator behind the displaced nasal bone)

Figure 4: Reduction using nasal bone forceps
2. Management of Open Nasal Bone Fractures
Under local or general anesthesia, perform conservative debridement first, preserving soft tissue as much as possible and removing foreign bodies. Insert a nasal airway tube, pack the nose with iodoform gauze, reduce the fracture to achieve bilateral symmetry, and suture the skin. External fixation with a molded collodion or thin metal splint should be maintained for 4–7 days. If nasal packing serves as an internal splint, replace it every 2–3 days and remove it after 7 days. Administer sufficient antibiotics and tetanus antitoxin (TAT). In cases of cerebrospinal fluid rhinorrhea, nasal packing is generally contraindicated.



