| disease | Stomach Cancer |
| alias | Carcinoma of Stomach |
Stomach cancer is a malignant tumor originating from the epithelial cells of the gastric mucosa, accounting for 95% of gastric malignancies. The incidence of stomach cancer is very high in our country, with its mortality rate ranking first among malignant tumors. The average national mortality rate for stomach cancer is as high as 20 per 100,000, with men being more affected than women at a ratio of approximately 3:1. The peak age of onset is between 50 and 60 years. The global annual incidence rate of stomach cancer is 17.6 per 100,000, with high rates in countries like Japan and Denmark, and lower rates in the United States and Australia. In China, coastal areas such as Shandong, Zhejiang, Shanghai, and Fujian are high-risk regions.
bubble_chart Epidemiology
The incidence and mortality rates of stomach cancer vary significantly among different countries and regions, with the ratio between high and low rates differing by up to 10 times. Countries such as Japan, Chile, Iceland, Austria, Finland, and Hungary are high-incidence areas, while regions like North America, India, Indonesia, Malaysia, and Egypt have lower incidence rates. China also has a high incidence of stomach cancer, particularly in the Hexi Corridor of Gansu, the Jiaodong Peninsula, and the coastal areas of Jiangsu and Zhejiang. Within the same country, there can be notable differences in incidence rates between different regions, with high-incidence areas having low-incidence spots and low-incidence areas having high-incidence spots. Epidemiological investigations are of great significance for studying the causes and mechanisms of stomach cancer.
It is currently believed that the following factors are related to the occurrence of stomach cancer:(1) Environmental factors: The significant differences in incidence rates among different countries and regions suggest a connection with environmental factors, with diet being the most important.
Salt may be one of the exogenous factors inducing stomach cancer, as countries with high salt intake among residents also have high stomach cancer incidence rates. Nitrosamine compounds have successfully induced stomach cancer in animals. Smoked fish and meat contain higher levels of 3,4-benzopyrene; moldy food contains more fungal toxins; rice processed with talc powder, whose chemical properties and structure are similar to asbestos fibers, is also considered carcinogenic.
(2) Genetic factors: The incidence of stomach cancer is higher in certain families. Some data indicate that stomach cancer occurs more frequently in people with blood type A than in those with blood type O.
(3) Immune factors: People with low immune function have a higher incidence of stomach cancer, possibly due to immune dysfunction and reduced immune surveillance against cancer, which plays a role in the development of stomach cancer.
(4) Precancerous changes: Precancerous changes refer to certain lesions with a strong tendency to become malignant. If not treated, these lesions may develop into stomach cancer. Precancerous changes include precancerous conditions and precancerous lesions.
1. Precancerous conditions of the stomach
(1) Chronic atrophic gastritis: There is a significant positive correlation between chronic atrophic gastritis and the incidence of stomach cancer.
(2) Pernicious anemia: 10% of patients with pernicious anemia develop stomach cancer, with an incidence rate 5-10 times higher than that of the normal population.
(3) Gastric polyps: Although adenomatous or villous polyps account for a small proportion of gastric polyps, their malignant transformation rate is 15-40%. Polyps larger than 2 cm have an even higher malignant transformation rate. Hyperplastic polyps are more common, but their malignant transformation rate is only 1%.(4) Remnant stomach: Cancer occurring in the remnant stomach after benign gastric surgery is called remnant stomach cancer. The incidence significantly increases after gastric surgery, especially 10 years post-operation.
(5) Benign gastric ulcer: Gastric ulcer itself is not a precancerous condition, but the mucosa at the ulcer margin is prone to intestinal metaplasia and malignant transformation.
(6) Giant gastric mucosal folds (Menetrier's disease): Serum protein is lost through the giant gastric mucosal folds, leading to hypoproteinemia and edema clinically. About 10% of cases may become cancerous.
2. Precancerous lesions of the stomach
(1) Dysplasia and anaplasia: The former, also known as atypical hyperplasia, is a reversible pathological cell proliferation caused by chronic inflammation, with a few cases potentially becoming cancerous. Gastric anaplasia has a higher chance of malignant transformation.
(2) Intestinal metaplasia: There are two types, small intestine type and large intestine type. The small intestine type (complete type) has characteristics of small intestine mucosa and is well-differentiated. The large intestine type (incomplete type) resembles large intestine mucosa and can be further divided into two subtypes: Type IIa, which secretes non-sulfated mucin, and Type IIb, which secretes sulfated mucin. Type IIb is closely related to the development of stomach cancer.
bubble_chart Pathological Changes(1) Location of stomach cancer occurrence: Stomach cancer can occur in any part of the stomach, with more than half occurring in the gastric antrum, lesser curvature, and anterior and posterior walls, followed by the cardia region, and relatively less in the gastric body region.
(2) Gross morphological classification
1. Early stomach cancer: Regardless of size, early lesions are limited to the mucosa and submucosa. It can be divided into three types: elevated type (polyp type), superficial type (gastritis type), and depressed type (ulcer type). Type II is further divided into three subtypes: IIa (elevated superficial type), IIb (flat superficial type), and IIc (depressed superficial type). The above types can have different combinations, such as IIc+IIa, IIc+III, etc. (Figure 1). Early stomach cancer with a diameter of 5-10mm is called small stomach cancer, and those with a diameter <5mm are called micro stomach cancer.
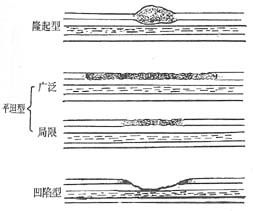
Figure 1 Schematic diagram of early stomach cancer classification
2. Intermediate and advanced stage stomach cancer: Also known as progressive stomach cancer, the cancerous lesion invades the muscular layer or the entire layer, often with metastasis. There are several types (Figure 2):
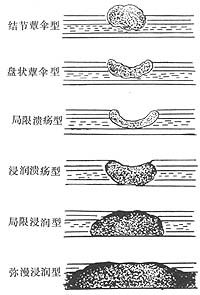
Figure 2 Schematic diagram of intermediate and advanced stage stomach cancer classification
(1) Fungating type (or polypoid type): Accounts for about 1/4 of advanced stage stomach cancer. The cancer is localized, mainly growing into the cavity, presenting as nodular or polypoid, with a rough surface resembling cauliflower, and central erosion or ulcer, also known as nodular fungating type (Color Figure 3). The cancer is disc-shaped, with raised edges and a central ulcer, called disc-shaped fungating type.

Figure 3 Intermediate and advanced stage stomach cancer (elevated type)
A mass protrudes into the gastric cavity from the posterior wall of the lesser curvature of the gastric antrum, slightly lobulated, with an uneven granular surface and visible erosion. The base of the mass is slightly narrow, presenting as a subpedunculated type, with no obvious infiltration in the surrounding mucosa.
(2) Ulcer type: Accounts for about 1/4 of advanced stage stomach cancer. It is further divided into localized ulcer type and infiltrative ulcer type. The former is characterized by localized cancer, disc-shaped, with central necrosis. Often has a large and deep ulcer; the ulcer base is generally uneven, with raised edges like a dike or crater, and the cancer infiltrates deeply, often accompanied by bleeding and perforation. The infiltrative ulcer type is characterized by infiltrative growth of the cancer, often forming a mass that infiltrates the surrounding and deep tissues, with central necrosis forming an ulcer, often invading the serosa or causing lymph node metastasis early.
(3) Infiltrative type: This type is also divided into two types, one is localized infiltrative type, where the cancer tissue infiltrates all layers of the gastric wall, mostly limited to the gastric antrum, the infiltrated gastric wall thickens and hardens, folds disappear, and there is usually no obvious ulcer or nodule. Infiltration limited to a part of the stomach is called "localized infiltrative type". The other is diffuse infiltrative type, also known as linitis plastica, where the cancer tissue spreads under the mucosa, invading all layers, with a wide range, causing the gastric cavity to shrink, the gastric wall to thicken and harden, the mucosa may still exist, with possible congestion and edema but no ulcer.
(4) Mixed type: Two or more of the above types coexist.
(5) Multiple cancers: The cancer tissue is multifocal and not connected. For example, stomach cancer occurring on the basis of atrophic gastritis may belong to this type, and is mostly in the upper part of the gastric body.
(3) Histological classification: According to the tissue structure, it can be divided into 4 types. ① Adenocarcinoma: Including papillary adenocarcinoma, tubular adenocarcinoma, and mucinous adenocarcinoma, which are divided into well-differentiated, moderately differentiated, and poorly differentiated according to their degree of differentiation; ② Undifferentiated carcinoma; ③ Mucinous carcinoma (i.e., signet ring cell carcinoma); ④ Special types of carcinoma: Including adenosquamous carcinoma, squamous cell carcinoma, carcinoid, etc.
According to histogenesis, it can be divided into two types. ① Intestinal type: The cancer originates from the epithelium of intestinal metaplasia, with better differentiation of the cancer tissue, and the gross morphology is mostly of the fungating type; ② Gastric type: The cancer originates from the native gastric mucosa, including undifferentiated carcinoma and mucinous carcinoma, with poorer differentiation of the cancer tissue, and the gross morphology is mostly of the ulcerative type and diffuse infiltrative type.
(4) Pathways of Spread
1. Direct Spread Infiltrative stomach cancer can directly spread along the mucous membrane or serous membrane into the stomach wall, esophagus, or duodenum. Once the cancer invades the serous membrane, it can easily infiltrate into surrounding adjacent organs or tissues such as the liver, pancreas, spleen, transverse colon, jejunum, diaphragm, greater omentum, and abdominal wall. When cancer cells detach, they can also implant in the abdominal cavity, pelvic cavity, ovaries, and rectovesical pouch.
2. Lymph Node Metastasis This accounts for 70% of stomach cancer metastases. Cancers in the lower part of the stomach often metastasize to the lymph nodes below the pylorus, below the stomach, and beside the abdominal aorta, while cancers in the upper part of the stomach often metastasize to the lymph nodes beside the pancreas, beside the cardia, and above the stomach. Advanced-stage cancers may metastasize to the lymph nodes around the main aorta and above the diaphragm. Since the abdominal lymph nodes are directly connected to the thoracic duct, metastasis to the left supraclavicular lymph nodes can occur.
3. Hematogenous Spread In some patients, cancer cells can be found in the peripheral blood. They can spread through the portal vein to the liver and can reach the lungs, bones, kidneys, brain, meninges, spleen, skin, and other sites.
bubble_chart Clinical Manifestations
(1) Symptoms More than 70% of early stomach cancer cases may be asymptomatic. Based on the pathogenesis, the symptoms of advanced stage stomach cancer can be divided into four aspects.
1. Energy consumption and metabolic disorders caused by cancer proliferation lead to decreased resistance, malnutrition, vitamin deficiency, etc., manifested as lack of strength, loss of appetite, nausea, weight loss, anemia, edema, fever, constipation, dry skin, and hair loss.
2. Stomach cancer ulceration can cause upper abdominal pain, gastrointestinal bleeding, perforation, etc. Stomach cancer pain is often gnawing, not clearly related to eating or worsening after eating. Some resemble the pain of peptic ulcers, which can be relieved by eating or antacids, and this condition can last for a long time, with the pain gradually worsening and becoming persistent. When the cancer bleeds, it manifests as positive fecal occult blood test, hematemesis, or black stool. 5% of patients experience major bleeding, and some may seek medical attention for the first time due to acute abdominal conditions such as bleeding or stomach cancer perforation.
3. Symptoms caused by the mechanical effects of stomach cancer, such as a feeling of fullness and heaviness due to poor stomach filling, as well as tastelessness, anorexia, pain, nausea, vomiting, etc. Stomach cancer near the cardia can invade the esophagus, causing hiccups and difficulty swallowing, while cancer near the pylorus can cause pyloric obstruction.
4. Symptoms caused by the spread and metastasis of cancer, such as ascites, hepatomegaly, jaundice, and metastasis to the lungs, brain, heart, prostate, ovaries, bone marrow, etc., causing corresponding symptoms.
(2) Signs Early stomach cancer may have no signs, and among the signs of mid to advanced stage cancer, upper abdominal tenderness is the most common. One-third of patients may have a palpable upper abdominal mass, which is hard and irregular, and may be tender. The detection of an abdominal mass depends on the location and size of the cancer and the thickness of the patient's abdominal wall. More cases of gastric antrum cancer may have a palpable abdominal mass.
Other signs are mostly caused by advanced stage stomach cancer or metastasis, such as an enlarged, hard, and irregular liver, jaundice, ascites, and enlarged lymph nodes in the left supraclavicular and left axillary regions. In male patients, a hard mass may be palpated in the upper part of the prostate during rectal examination, and in female patients, an enlarged ovary may be palpated during vaginal examination. Other rare signs include nodules on the skin and linea alba, enlarged inguinal lymph nodes, and fever in advanced stages, often presenting as cachexia. In addition, paraneoplastic syndromes of stomach cancer, including thrombophlebitis, acanthosis nigricans, and dermatomyositis, may have corresponding signs.
bubble_chart Auxiliary Examination
(1) Gastrointestinal X-ray examination is the primary method for diagnosing stomach cancer. It includes imaging at different degrees of distension to display the mucosal patterns, such as compression imaging and double-contrast methods. Particularly, the barium-air double-contrast method is valuable for detecting small lesions in the gastric wall.
1. X-ray manifestations of early stomach cancer: Under appropriate compression or double-contrast, the elevated type often shows small filling defects with an irregular surface, a slightly wider base, and thickened, disordered nearby mucosa, which can be distinguished from benign polyps (Figure 4).
|
|
|
| A. Gastric filling film: Shows a slight depression on the greater curvature of the prepyloric region of the stomach, with no visible filling defect. | B. Gastric compression film: Shows small filling defects in the stomach, with thickened mucosa in the gastric antrum. Pathological examination revealed early stomach cancer. |


Figure 4: Early elevated type stomach cancer
Superficial type (Figure 5): The mucosa is flat, with visible granular hyperplasia or slight discoid elevation. Some patients may show small areas of barium abdominal mass or slight protrusion during filling. The peristalsis in the affected area generally remains, but the gastric wall is slightly stiffer than normal.
|
|
|
| A. Gastric filling film: Shows slight irregularity at the angular notch of the lesser curvature of the stomach. | B. Double-contrast film: Shows thickened mucosa in the gastric antrum and lesser curvature, with flattened mucosa near the angular notch. |


Figure 5: Early flat type stomach cancer
Depressed type (Figure 6): Shows shallow niche shadows, mostly with rough and uneven bottoms. The gastric wall may be slightly stiffer than normal, but peristalsis and contraction remain. Under compression or double-contrast, the depressed area may show a faint, irregular barium abdominal mass, with adjacent mucosal folds often showing club-shaped interruptions.
|
| |
A. Gastric filling film shows localized irregularity on the vertical part of the lesser curvature of the stomach | |
|
|
|
B. Gastric compression tablet shows limited residual barium in small fragments, with thickening of the nearby mucous membrane, and the mucous membrane of the gastric antrum is also thickened. | C. Gastrectomy specimen: The arrow points to the depressed area of stomach cancer. |



Figure 6: Early depressed-type stomach cancer.
2. X-ray manifestations of mid to advanced stage stomach cancer: Fungating type (Figure 7): It appears as a filling defect protruding into the gastric cavity, generally large, with irregular or lobulated contours, a broad base, and often irregular niches due to ulcers within the filling defect. The gastric mucosal folds around the filling defect are interrupted or disappeared. The gastric wall is slightly rigid.

Figure 7: Fungating-type stomach cancer in the gastric antrum.
Shows irregular filling defect in the gastric antrum, polypoid in appearance.
Ulcerative type (Figure 8): Mainly manifested as niche shadows (see Figure 8), with irregular ulcer edges, showing finger-like impressions and a surrounding mound, with nodular hyperplasia of the surrounding folds, sometimes abruptly interrupted at the mound. The mixed type is commonly dominated by ulcers, accompanied by proliferative and infiltrative changes.
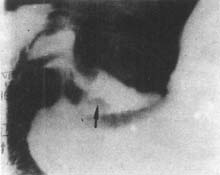
Figure 8: Ulcerative-type stomach cancer in the gastric antrum.
Irregular shadow on the lesser curvature of the gastric antrum, with polypoid hyperplasia around, forming finger-like impressions (↑) and fissures.
Infiltrative type (Figure 9): The localized type is characterized by abnormally thickened or disappeared mucosal folds, localized gastric wall rigidity, fixed narrowing of the gastric cavity, and double shadows of the gastric wall on films taken at different times in the same position, indicating overlapping contours of normal peristaltic gastric wall and rigid gastric wall. The diffuse infiltrative type shows flattened or disappeared mucosal folds, significantly reduced gastric cavity, and the entire gastric wall is rigid with no peristaltic waves visible (Figure 10).

Figure 9: Infiltrative-type stomach cancer in the gastric antrum.
Shows narrowing of the gastric antrum caused by the cancer.
|
|
|
A. The gastric cavity is significantly reduced, normal mucosal folds disappeared, showing granular shadows. | B. The stomach cannot be filled, easily emptied, and the gastric contour is still smooth. |


Figure 10: Infiltrative-type stomach cancer (presenting as linitis plastica).
(2) Endoscopy: It allows direct observation of various parts of the stomach and has significant diagnostic value for stomach cancer, especially early-stage stomach cancer.
1. Early stomach cancer - Elevated type (Color Figure 11) mainly manifests as a local mucosal elevation protruding into the gastric cavity, with a stalk or broad base, and a rough surface, sometimes presenting as papillary or nodular, with possible erosion on the surface. The superficial type shows irregular borders, indistinct boundaries, and local mucosal roughness, slightly elevated or depressed, with a faded or reddened surface, and possible erosion. This type of lesion is most prone to fistula disease. The depressed type has a more obvious ulcer, with the depression often exceeding the mucosal layer (Color Figure 12). The above types can coexist to form a mixed type of early stomach cancer.

Figure 11 Early stomach cancer (elevated type)
There is a hemispherical polyp-like elevation on the greater curvature of the middle part of the stomach body, with a smooth surface, hard texture, about 1.5 cm in diameter, broad base, intact surrounding mucosa, no edema, no infiltration.

Figure 12 Early stomach cancer (superficial ulcer type)
There is an elevation on the posterior wall near the pyloric region, partially nodular, pale in color, with an irregular shallow ulcer in the center, pathologically confirmed as adenocarcinoma.
2. Mid to advanced stage stomach cancer - Often exhibits typical manifestations of stomach cancer, making endoscopic diagnosis not difficult. The elevated type has a larger lesion diameter, irregular shape, resembling a cauliflower or chrysanthemum flower.
(3) Gastric juice examination - About half of stomach cancer patients have achlorhydria. The lactic acid content in basal gastric acid may exceed normal levels (100μg/ml). However, gastric juice analysis is not very significant for the diagnosis of stomach cancer.
(4) Biological and biochemical examinations - Including immunological reactions of cancer, measurement of special chemical components in the body, and enzyme reactions, etc. Such as serum pepsinogen I and the ratio of pepsinogen I/II; CEA, CA19-9, CA 125 and other carcinoembryonic antigens and monoclonal antibody detection, but these tests have high false positives and false negatives, with low specificity.
(1) Symptoms Early manifestations include upper abdominal discomfort, which is present in about 80% of patients. Nearly 50% of stomach cancer patients experience significant loss of appetite or anorexia. In the advanced stage, symptoms such as lack of strength, back pain, and obstruction-related nausea, vomiting, and difficulty eating may occur. When the tumor surface ulcerates, hematemesis and black stools may appear.
(2) Signs In the early stages, there are no specific signs. In the advanced stage, an upper abdominal mass may be palpable, and a rectal examination may reveal a mass. Enlargement of the left supraclavicular lymph nodes may also be observed, along with signs of anemia, weight loss, ascites, and other cachexia manifestations.
(3) Laboratory Tests In early suspected stomach cancer, there may be low or absent free gastric acid. Indicators such as hematocrit, hemoglobin, and red blood cell count may decrease, and stool occult blood may be positive. Total hemoglobin may be low, with an inverted albumin/globulin ratio. Electrolyte imbalances and acid-base disturbances may also be detected.
(4) X-ray Findings Double-contrast barium studies can clearly show the gastric contour, peristalsis, mucosal morphology, and emptying time, as well as the presence of filling defects or niches. The accuracy rate of this examination is nearly 80%.
(5) Fiberoptic Endoscopy This is the most direct, accurate, and effective diagnostic method for stomach cancer.
(6) Exfoliative Cytology Some scholars recommend this examination for clinically and radiologically suspected stomach cancer during seasonal epidemics.
(7) B-ultrasound This can assess whether there is metastasis to surrounding solid organs.
(8) CT Scan This helps to understand the extent of gastric tumor invasion, its relationship with surrounding organs, and the possibility of resection.
(9) Immunological Tests These include CEA, FSA, GCA, and YM globulin tests. {|108|}
bubble_chart Treatment Measures
The treatment of stomach cancer is the same as that of other malignant tumors, with surgical treatment being the preferred method. It should be reasonably combined with chemotherapy, radiotherapy, Chinese medicine Chinese medicinals, and immunotherapy according to the situation.
Based on the TNM staging, the current comprehensive treatment plan is roughly as follows.
Stage I stomach cancer is considered early-stage stomach cancer, with surgical resection as the main treatment. For individual cases of type IIa and IIc that invade the submucosal layer and have lymph node metastasis, chemotherapy should be appropriately combined.
Stage II stomach cancer is considered intermediate-stage [second stage] stomach cancer, with surgical resection as the main treatment. Some cases may require adjuvant chemotherapy or immunotherapy.
Stage III stomach cancer often invades surrounding tissues and shows extensive lymph node metastasis. Although surgical resection is the main treatment, it should be combined with chemotherapy, radiotherapy, immunotherapy, and Chinese medicine Chinese medicinals.
Stage IV stomach cancer is already in the advanced stage, and non-surgical therapy is often used. For cases suitable for surgery, the primary and metastatic lesions should be resected as much as possible, combined with chemotherapy, radiotherapy, immunotherapy, and Chinese medicine Chinese medicinals.
(1) Surgical treatment is divided into radical surgery, palliative surgery, and bypass surgery.
1. Radical surgical resection: This concept is relative, meaning that the tumor is judged to have been completely removed, achieving a therapeutic effect. In reality, only a portion of cases can be cured.
2. Palliative resection: This refers to cases where the tumor is judged to be impossible to completely remove, but the main tumor mass can be resected. Resection can alleviate symptoms, prolong life, and create conditions for further comprehensive treatment.
3. Bypass surgery: This is mainly used for cases with pyloric obstruction that cannot be surgically removed. Gastrojejunostomy can relieve the obstruction.
(2) Radiotherapy
1. Preoperative radiotherapy: This refers to local irradiation before surgery for certain advanced stomach cancers with clinically palpable masses to improve the resection rate. The dosage is 200cGY per session, 5 sessions per week, for a total of 4 weeks, with a total dose of 4000cGY. Surgery is performed 10-14 days after stopping radiotherapy. This can increase the local resection rate but does not affect the degree of lymph node metastasis. Preoperative radiotherapy takes 6 weeks, so its impact on 5-year survival is difficult to estimate.
2. Intraoperative radiotherapy: This refers to a single high-dose irradiation of the surgical field centered on the abdominal stirred pulse after tumor resection and before gastrointestinal anastomosis, with a dose of 3000-3500cGY. This can improve the 5-year survival rate of advanced stomach cancer by about 10%. During surgery, the intestines must be isolated from the irradiation field to prevent radiation complications.
3. Postoperative radiotherapy: Most scholars believe it is ineffective.
(3) Chemotherapy: Except for early-stage stomach cancer, other advanced stomach cancers should undergo appropriate chemotherapy.
1. Systemic chemotherapy: The chemotherapy plan is determined clinically, considering factors such as tumor pathology type, location, and stage. Stomach cancer is mostly adenocarcinoma, and drugs such as 5-FM, MMC, ADM, and MeCCNu are often used. In the first year after surgery, three courses of chemotherapy should be administered, each lasting about 2 months, with a 2-month break between courses. In the second and third years, two courses per year are administered, and in the fourth and fifth years, one course per year is administered. Chemotherapy is not necessary after five years.
Common chemotherapy regimens:
(1) FAM: 5-Fu 500mg IV on days 1, 8, and 15
ADM 30-50mg IV on day 1
MMC 4-10mg IV on day 1
21 days as one cycle.
2. Intraperitoneal chemotherapy: This can be done by placing a catheter in the abdominal cavity after surgery or by implanting a chemotherapy pump and catheter for chemotherapy. This increases local concentration.
(4) Immunotherapy: Immunotherapy combined with chemotherapy can prolong the patient's life. Common drugs include interferon, IL-2, and BCG.
(5) Chinese medicine Chinese medicinals: The main focus is on strengthening the body. It can counteract the side effects of radiotherapy, increase white blood cells and platelets, regulate gastrointestinal function, and improve the body's resistance.
The prognosis of stomach cancer depends on the location and extent of the tumor, histological type, depth of gastric wall invasion, metastasis status, host response, and surgical approach.
Since the cause of stomach cancer is not yet clear, there are no specific prevention methods. In addition to paying attention to dietary hygiene and avoiding or reducing the intake of potential carcinogens, it is advisable to consume more vegetables and fruits rich in vitamin C. For so-called precancerous lesions, close follow-up is necessary to detect changes early and provide timely treatment.
Stomach cancer can lead to complications such as bleeding, perforation, obstruction, gastrointestinal fistula, perigastric adhesions, and abscess formation.
Stomach cancer must be differentiated from gastric ulcers, simple gastric polyps, benign tumors, fleshy tumors, and chronic gastric inflammation. Sometimes it also needs to be distinguished from gastric fold hypertrophy, giant fold disease, gastric mucosal prolapse, pyloric muscle hypertrophy, and severe gastric fundal varices. The differential diagnosis mainly relies on X-ray barium meal imaging, gastroscopy, and pathological biopsy.