| disease | Orbital Floor Fracture |
| alias | Fracture of Orbital Floor |
Orbital fractures can occur alone or in conjunction with fractures of other maxillofacial bones, such as zygomatic fractures, frontal bone fractures, or maxillary Le Fort II and III fractures. Clinically encountered orbital fractures include orbital floor fractures, supraorbital rim fractures, orbital roof fractures, and fractures of the medial and lateral orbital walls. Among these, orbital floor fractures present certain distinctive features in diagnosis and treatment.
bubble_chart Etiology
The orbital floor is fragile and primarily composed of the orbital process of the maxilla, which forms the upper wall of the maxillary sinus, with the zygomatic bone's orbital process located laterally. The orbital floor slopes upward and backward, with its posterior region being the most fragile area, traversed by the infraorbital canal and infraorbital fissure. This area connects with the lamina papyracea of the ethmoid bone, forming the inferomedial wall of the orbital floor, which is as thin as paper (Figure 2). When a fracture occurs in the midface due to external impact, the orbital floor is subjected to force, causing a sharp increase in intraorbital pressure. This can lead to a fracture of the orbital floor, also known as a blowout fracture. Since the maxillary sinus lies below the orbital floor, such fractures often result in herniation of orbital contents into the maxillary sinus (Figure 3).
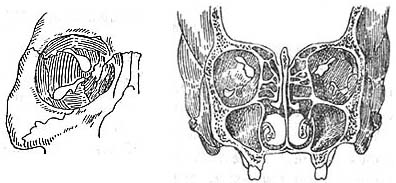
Figure 2 Anatomical relationships of the orbit
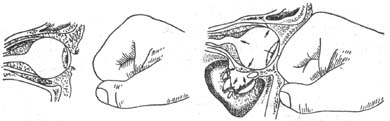
Figure 3 A blunt force impact on the orbital rim causes a sudden increase in intraorbital pressure, resulting in a blowout fracture of the fragile orbital floor.
bubble_chart Clinical Manifestations
1. Periorbital static blood and swelling may be caused by subcutaneous and subconjunctival hemorrhage around the orbit. If there is significant intraorbital hemorrhage, it may lead to proptosis. A step deformity is often palpable at the infraorbital margin, accompanied by tenderness.2. Enophthalmos is an important sign of orbital floor fracture. The main causes of enophthalmos are: ① Due to the orbital floor fracture, the orbital contents, including the eyeball, are displaced downward or herniated into the maxillary sinus cavity; ② The displaced orbital floor fracture fragments enlarge the orbital cavity, resulting in insufficient orbital fat to support the eyeball (Figure 4).
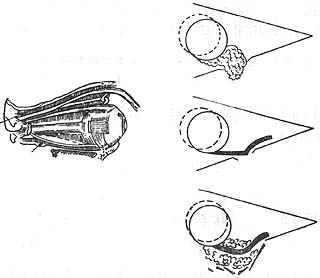
Figure 4 Causes of enophthalmos in blowout fracture
3. Diplopia In blowout fractures, the orbital contents, including the inferior rectus muscle, inferior oblique muscle, and orbital septa, are displaced downward, leading to restricted vertical movement of the extraocular muscles and resulting in diplopia. If the oculomotor nerve is injured, it can also cause diplopia.
4. Infraorbital numbness Fracture fragments from an orbital floor fracture often injure or compress the infraorbital nerve, causing numbness in the area supplied by this nerve.
1. Medical History: Patients with a history of blunt trauma to the eye from an object larger than the orbit or injuries causing multiple fractures in the midface should be evaluated for possible orbital floor fractures.
2. Midface Fracture with Enophthalmos and Diplopia: Patients with midface fractures presenting with enophthalmos and diplopia.
3. Positive Forced Duction Test: After topical anesthesia with tetracaine, use ophthalmic forceps with teeth to grasp the inferior rectus tendon through the conjunctiva and perform a forced duction test. If upward movement of the eye is restricted, the test is positive, indicating inferior rectus entrapment (Figure 1).
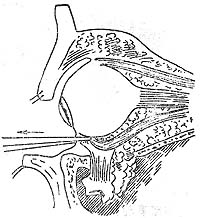
Figure 1: Forced duction test using forceps to grasp the inferior rectus muscle.
4. X-ray Examination: Water's view or tomography can be selected to assess the orbital cavity, orbital floor, and maxillary sinus.
bubble_chart Treatment Measures
Surgical treatment should be performed promptly. The optimal timing for surgery is approximately 1 week after the injury, as performing surgery too early may result in unresolved tissue swelling in the injured area, while delaying it may lead to malunion or scar formation, both of which can compromise satisfactory outcomes.
The objectives of the surgery are to reposition the incarcerated extraocular muscles and orbital fat, restore orbital volume and ocular motility, and improve enophthalmos and diplopia.
Surgical technique: A transverse incision is made below the eyelash of the lower eyelid, cutting through the skin and orbicularis oculi muscle while avoiding the orbital septum. Dissection is carried downward along the orbital surface to the orbital rim. Below the orbital rim, the periosteum is incised horizontally, and the orbital floor periosteum is elevated along the bone surface to expose the orbital floor fracture site. Care must be taken to protect the infraorbital nerve. Meticulous and thorough dissection is performed to free the inferior rectus muscle and orbital contents from incarceration and reposition them into the orbit. A traction test is conducted to ensure unrestricted eye movement. If there is a fracture of the infraorbital rim, it should be reduced and fixed with interosseous wiring. For bony defects in the orbital floor, bone grafts or substitutes can be implanted to reconstruct the orbital floor.



