| disease | Pelvic Rectal Abscess |
| alias | Peripheral Abscess |
Acute purulent infection occurring in or around the soft tissues surrounding the anal canal and rectum, leading to the formation of an abscess, is referred to as a perianal or perirectal abscess. It is characterized by spontaneous rupture or often developing into an anal fistula after surgical incision and drainage. This is a common anorectal disease and represents the acute phase of inflammatory pathological processes in the anal canal and rectum, with anal fistula being the chronic phase. Common pathogenic bacteria include Escherichia coli, Staphylococcus aureus, Streptococcus, and Pseudomonas aeruginosa, occasionally anaerobic bacteria and Mycobacterium tuberculosis, often presenting as mixed infections. Although pelvic rectal abscesses are rare, they are significant. Due to the lack of obvious local symptoms perceived by the patient and the presence of prominent systemic symptoms, early diagnosis is often delayed.
bubble_chart Diagnosis
Infection is often caused by proctitis, rectal ulcers, or rectal trauma, and can also result from the spread of intermuscular abscesses or ischiorectal fossa abscesses. The onset is slow, with early symptoms limited to a sense of fullness in the rectum, especially discomfort during defecation, and sometimes difficulty urinating. Examination: There is usually no abnormality around the anus, but a digital rectal exam may reveal infiltration, tenderness, swelling, or even fluctuation on the anterolateral wall of the upper rectum. Diagnosis primarily relies on needle aspiration of pus, using a finger in the rectum for guidance while inserting the needle through the perianal skin. If necessary, an anal ultrasound can be performed to assist in diagnosis.
bubble_chart Treatment MeasuresThe surgical incision is similar to that for an ischiorectal abscess, but slightly more posterior and somewhat longer. The left index finger is inserted into the rectum to locate the abscess and guide the procedure. With the other hand, a curved clamp is passed through the skin incision, penetrating the levator ani muscle to enter the abscess cavity. The clamp is then spread in an anteroposterior direction to drain the pus. Next, the right index finger is inserted into the abscess cavity to separate the fibers of the levator ani muscle and enlarge the drainage. After irrigating the abscess cavity, a soft rubber tube or cigarette drain is placed and secured with a safety pin to prevent it from slipping into the cavity (Figure 1).
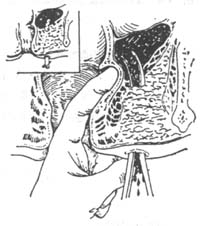
Figure 1 Incision and drainage of a pelvirectal abscess.


